



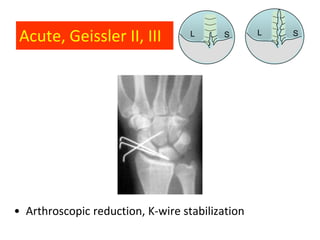
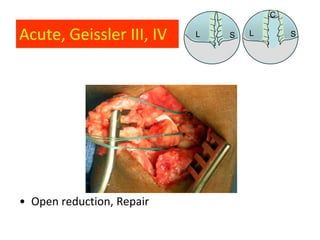

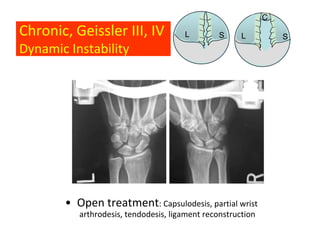
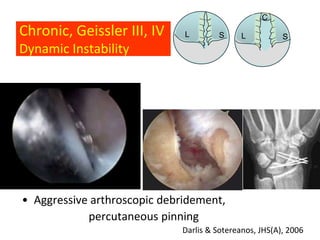
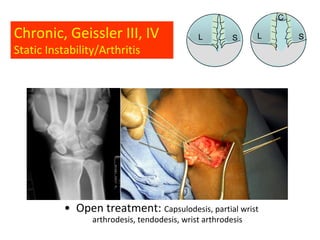

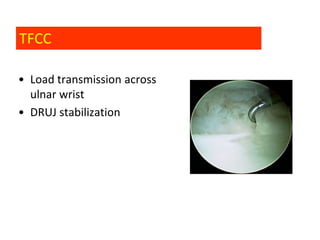

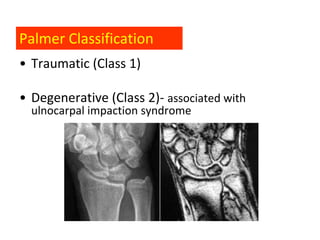
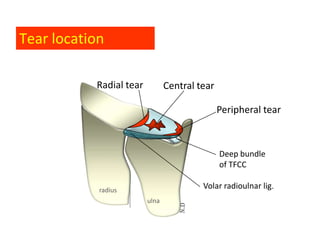

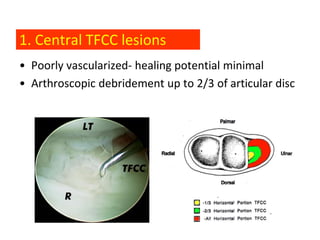

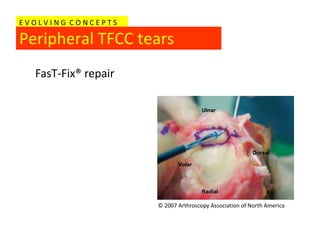
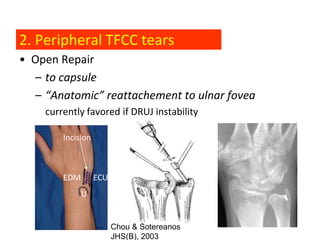


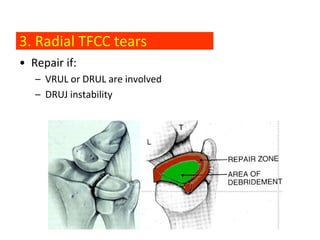
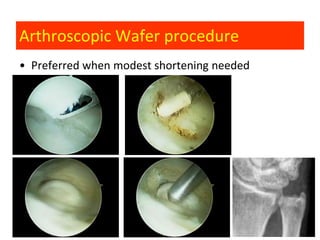
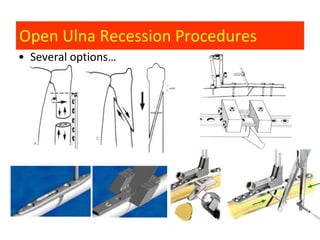
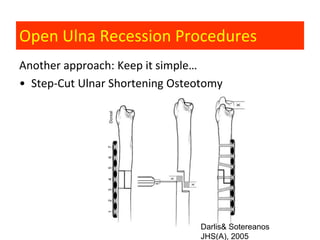

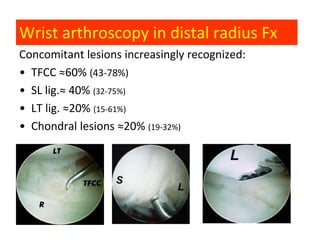







This document discusses wrist arthroscopy techniques and indications. It covers management of scapholunate ligament injuries, triangular fibrocartilage complex tears, and distal radius fractures. Key points include: - Arthroscopic debridement and repair are used for acute vs chronic scapholunate ligament injuries. - Central triangular fibrocartilage complex tears are debrided while peripheral tears can be repaired arthroscopically or openly. - Ulnocarpal impaction syndrome is treated with wafer resection or ulna shortening osteotomy. - Arthroscopy can aid reduction and detection of injuries for some distal radius fractures.
































































































