Laryngopharyngeal reflux (LPR) involves the backward flow of gastric contents into the laryngopharynx, often causing symptoms like hoarseness and cough, and is commonly associated with gastroesophageal reflux disease (GERD). Diagnosis is typically made through clinical evaluation and may involve a dual sensor pH probe, while treatment options range from lifestyle modifications to medications like proton pump inhibitors and, in some cases, surgery. Key risk factors include GERD, smoking, and alcohol, and the condition often presents without typical heartburn symptoms seen in GERD.
What is theLPR
is the retrograde movement of gastric
contents (acid and enzymes such as
pepsin) into the laryngopharynx leading to
symptoms referable to the
larynx/hypopharynx.
4.
60% ofpatients with GERD have LPR.
Damage is caused by the acidic gastric juice,
pepsin, bile salts, bacteria and pancreatic
proteolytic enzymes
5.
GERD: anabnormal amount of reflux up
through the lower sphincters and into the
esophagus.
LPRD: when the reflux passes all the way
through the upper sphincter reaching the
larynx and pharynx without belching or vomiting
7.
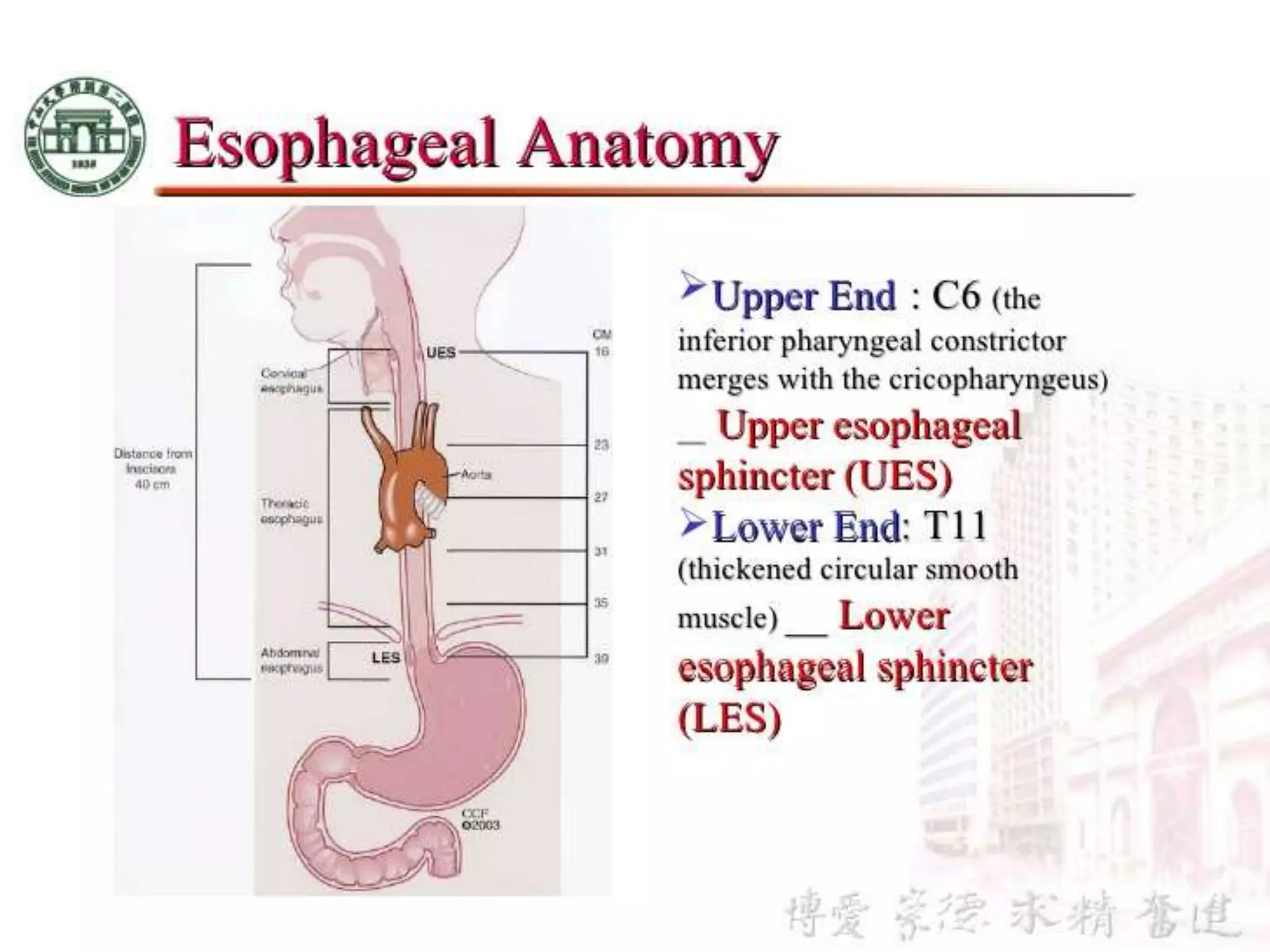
Upper esophagealsphincter :
The upper esophageal sphincter (UES) is composed of the
cricopharyngeus (CP), thyropharyngeus (TP; inferior pharyngeal
constrictor [IPC] in humans), and cranial cervical esophagus. All
3 muscles may at times function to maintain tone in the UES, but
only the CP contracts and relaxes in all physiologic states
consistent with the UES, it’s 3 cm in length
Lower esophageal sphincter :
Thickened circuler smooth muscle
3 cm in length
Regardless ofthe pathway, factors such
as the resting tone of the upper and lower
esophageal sphincters (UES and LES)
and the duration and magnitude of
increases in intraabdominal pressure are
important to the creation of the refluxate
bolus.
CLINICAL
MANIFESTATIONS
Hoarseness –70%
Voice fatigue, breaking of the voice
Cough – 50%
Globus pharyngeus – 47%
Frequent throat clearing, dysphagia, sore throat,
wheezing, laryngospasm, halitosis
Reinke’s edema : swelling of the vocal cords due
to fluid (edema) collected within the Reinke's
space “ a potential space between the vocal
ligament and the overlying mucosa “
11
Patterns and Mechanismof LPR
and GERD
13
LPR
No heartburn
Daytime (“upright”)
refluxers
Normal esophageal
motility
Normal acid
clearance
Majority without
esophagitis
GERD
Heartburn
Nocturnal (“supine”)
refluxers
Esophageal
dysmotility
Prolonged acid
clearance
Can present with
esophagitis
14.
DIAGNOSIS
There issignificant controversy over the appropriate way to
diagnose LPR and there is no test that is both easy to perform
and highly reliable.
Clinical diagnosis — common LPR complaints with
laryngoscopic findings associated with LPR
Dual sensor pH probe — The 24-hour dual sensor pH probe is
considered by many to be the gold standard for diagnosing LPR
Trial of therapy
Molecular and histologic evaluation — salivary epidermal
growth factor (EGF), immunologic markers, laryngeal mucosa
gene expression, and histologic changes.
Laryngoscopic Findings
Red,irritated arytenoids
Red, irritated larynx
Small laryngeal ulcers
Swelling of the VF
Granulomas in the larynx
pseudosulcus
17.
Therapeutic Trial forLPR
H2 receptor blockers
Work great for GERD
Proton pump inhibitors
Must use double dose PPI for therapeutic trial
Duration: 2 weeks – 6 months (one month should be
sufficient to see improvement
May still fail…
Remember: Non-acid reflux!
17
18.
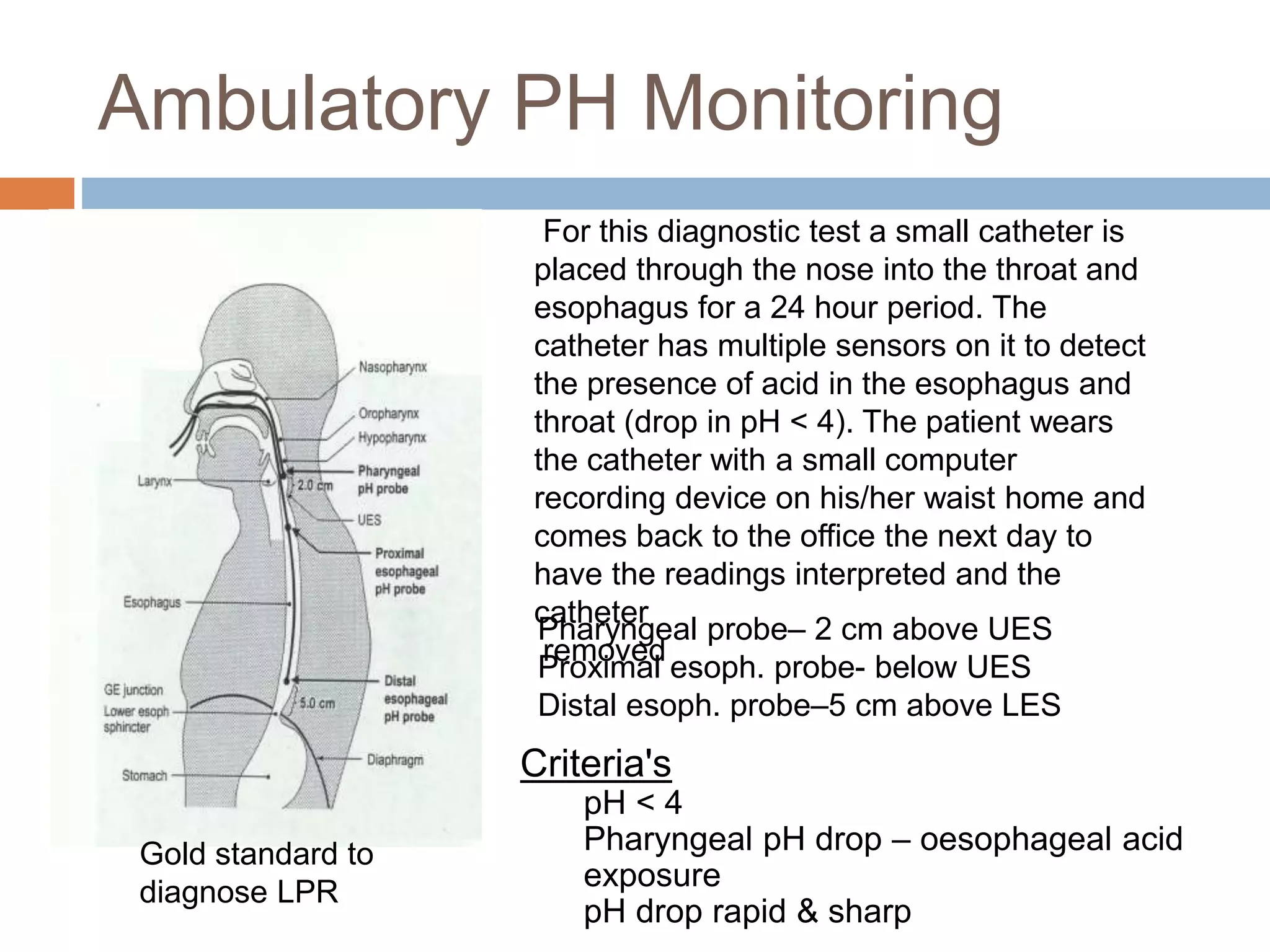
Ambulatory PH Monitoring
18
Pharyngealprobe– 2 cm above UES
Proximal esoph. probe- below UES
Distal esoph. probe–5 cm above LES
Gold standard to
diagnose LPR
Criteria's
pH < 4
Pharyngeal pH drop – oesophageal acid
exposure
pH drop rapid & sharp
For this diagnostic test a small catheter is
placed through the nose into the throat and
esophagus for a 24 hour period. The
catheter has multiple sensors on it to detect
the presence of acid in the esophagus and
throat (drop in pH < 4). The patient wears
the catheter with a small computer
recording device on his/her waist home and
comes back to the office the next day to
have the readings interpreted and the
catheter
removed
19.
Treatment
Antireflux therapy
PhaseI : Lifestyle-dietary modification
Antacid therapy
Phase II : Prokinetic
H2-blockers, PPI
Phase III : Antireflux surgery
19
20.
Lifestyle modifications
Stopsmoking
Elevate the head of the bed on blocks(15-
20cm)
Reduce body weight
Avoid tight-fitting clothing
Avoid lying down after meals
20
21.
Dietary modification
Avoidfat, caffeine, chocolate, mints,
carbonated drinks, fat, mints chocolate,
milk product, onion, cucumber
Avoid alcohol
Avoid overeating
Avoid ingestion of food and drink 2 hours
before bed time 21



![ Upper esophageal sphincter :
The upper esophageal sphincter (UES) is composed of the
cricopharyngeus (CP), thyropharyngeus (TP; inferior pharyngeal
constrictor [IPC] in humans), and cranial cervical esophagus. All
3 muscles may at times function to maintain tone in the UES, but
only the CP contracts and relaxes in all physiologic states
consistent with the UES, it’s 3 cm in length
Lower esophageal sphincter :
Thickened circuler smooth muscle
3 cm in length](https://image.slidesharecdn.com/laryngopharyngealrefluxlpr-180820193948/75/Laryngo-pharyngeal-reflux-lpr-7-2048.jpg)