Downloaded 36 times
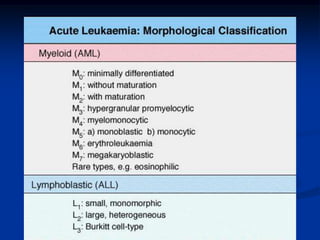
![II. Acute Myeloid Leukaemia (AML)
[ FAB]
M0 AML . . . Poorly differentiated
M1 AML . . . Without Maturation
M2 AML . . . With Maturation
M3 AproL . . . Promyelocytic
M4 AMML . . . MyeloMonocytic
M5 AMOL . . . Monocytic
M6 A. ErythroLeukaemia
M7 A. Megakaryoblastic L
Age groups : ALL – mostly in children
AML – mostly in Adults](https://image.slidesharecdn.com/acuteleukemia-140330163435-phpapp02/85/Acute-leukemia-11-320.jpg)

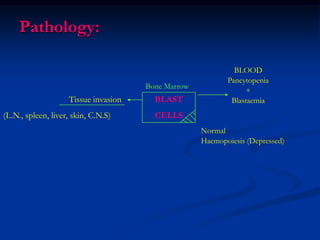
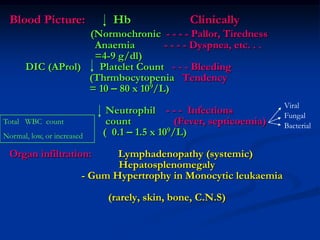
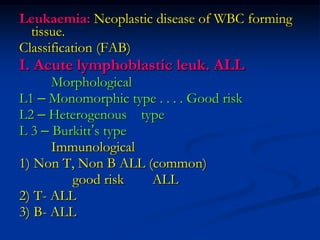
Leukaemias are malignant diseases of white blood cells that are classified as either acute or chronic. The main types are acute lymphoblastic leukemia (ALL), which mostly affects children, acute myeloid leukemia (AML), which mostly affects adults, chronic lymphocytic leukemia (CLL), and chronic myeloid leukemia (CML). The pathology involves an accumulation of immature blast cells in the bone marrow that suppress normal blood cell production, leading to bone marrow failure and the major clinical symptoms of fatigue, infections, and bleeding tendencies. The principle cause is believed to be acquired mutations in transcription factors that regulate blood cell differentiation.























































































