Download to read offline












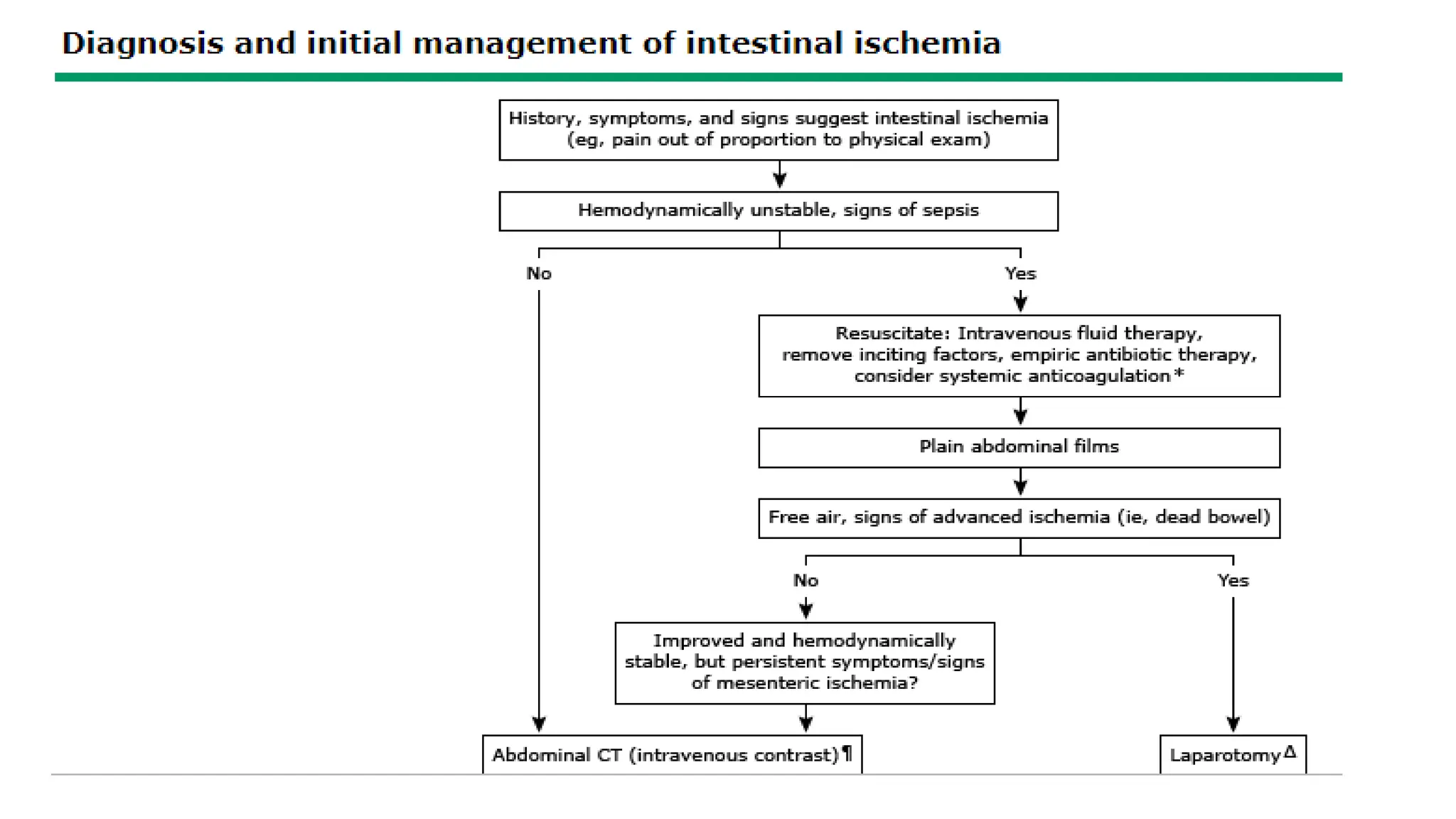

























Acute mesenteric ischemia is a life-threatening condition caused by sudden interruption of blood flow to the intestine. It has a high mortality rate of 60-80% if not treated promptly. The mesentery was recently recognized as a new organ. Diagnosis involves imaging studies like CT angiography to identify blockages or narrowing of mesenteric arteries. Initial management focuses on resuscitation, antibiotics, and pain control. Definitive treatment involves surgical exploration to assess bowel viability, identify the cause, perform revascularization if possible, and resect non-viable bowel. Prognosis depends on factors like age, time to treatment, and extent of necrosis - outcomes are better if revascularization is done within























































































