Definitions
Intestinal Obstructionis defined as
partial or complete blockage of the
bowel that results in the failure of
intestinal contents to pass.
5.
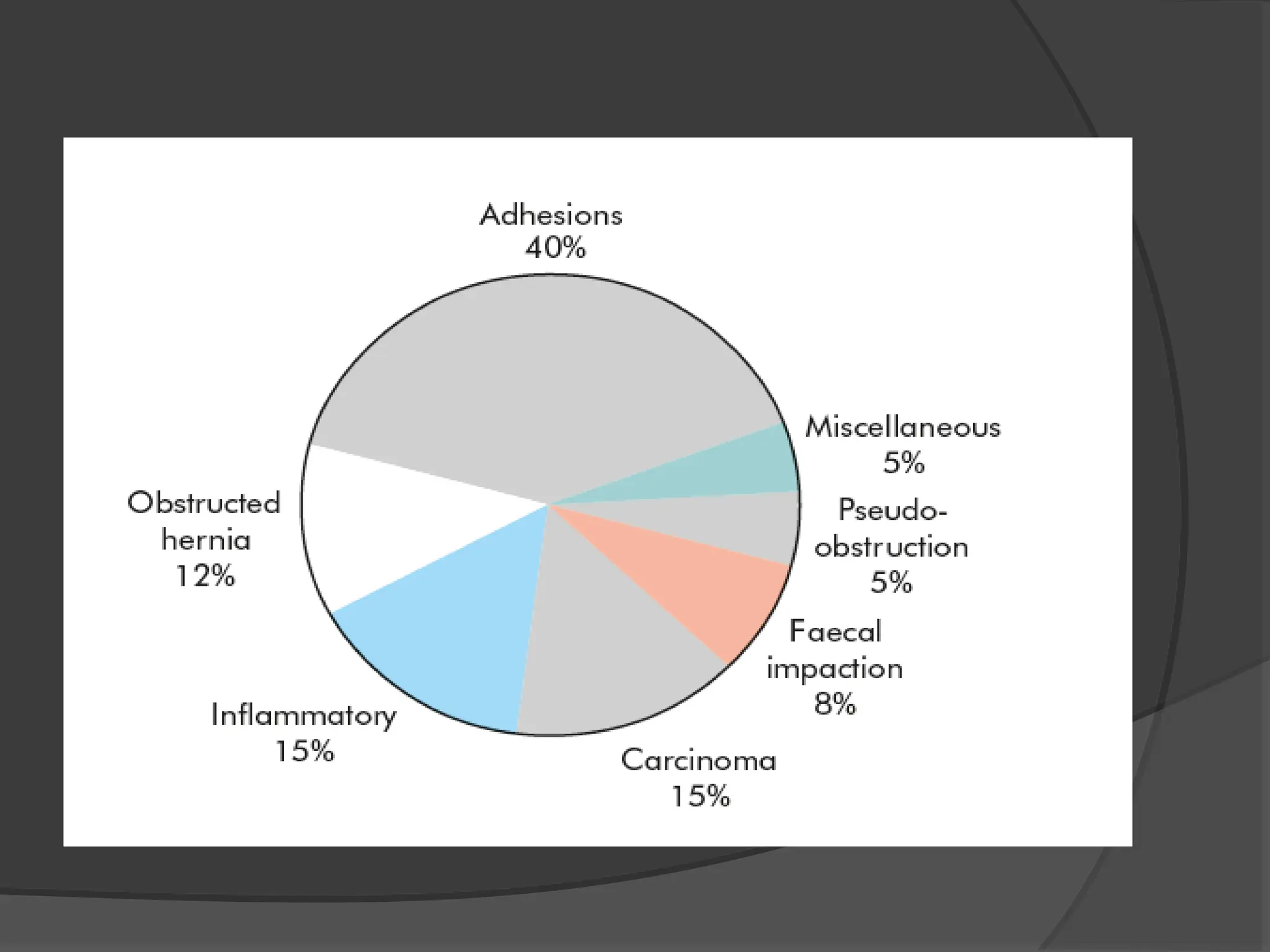
Intestinal obstructionis a common surgical
emergency & because of its serious nature it
demands early diagnosis & speedy relief.
1- Dynamic:- where peristalsis is working
against a mechanical obstruction ( acute or
chronic).
2- Adynamic:- this may occur in two forms:-
a- Absent peristalsis: - paralytic ileus.
b- Non-propulsive peristalsis: - Mesenteric
vascular occlusion.
6.
Intestinal obstruction canbe
classified into 2 types
Dynamic Adynamic
Peristalsis is working against a
mechanical obstruction. It may
accrue in an acute or chronic
form. “Mechanical Obstruction”
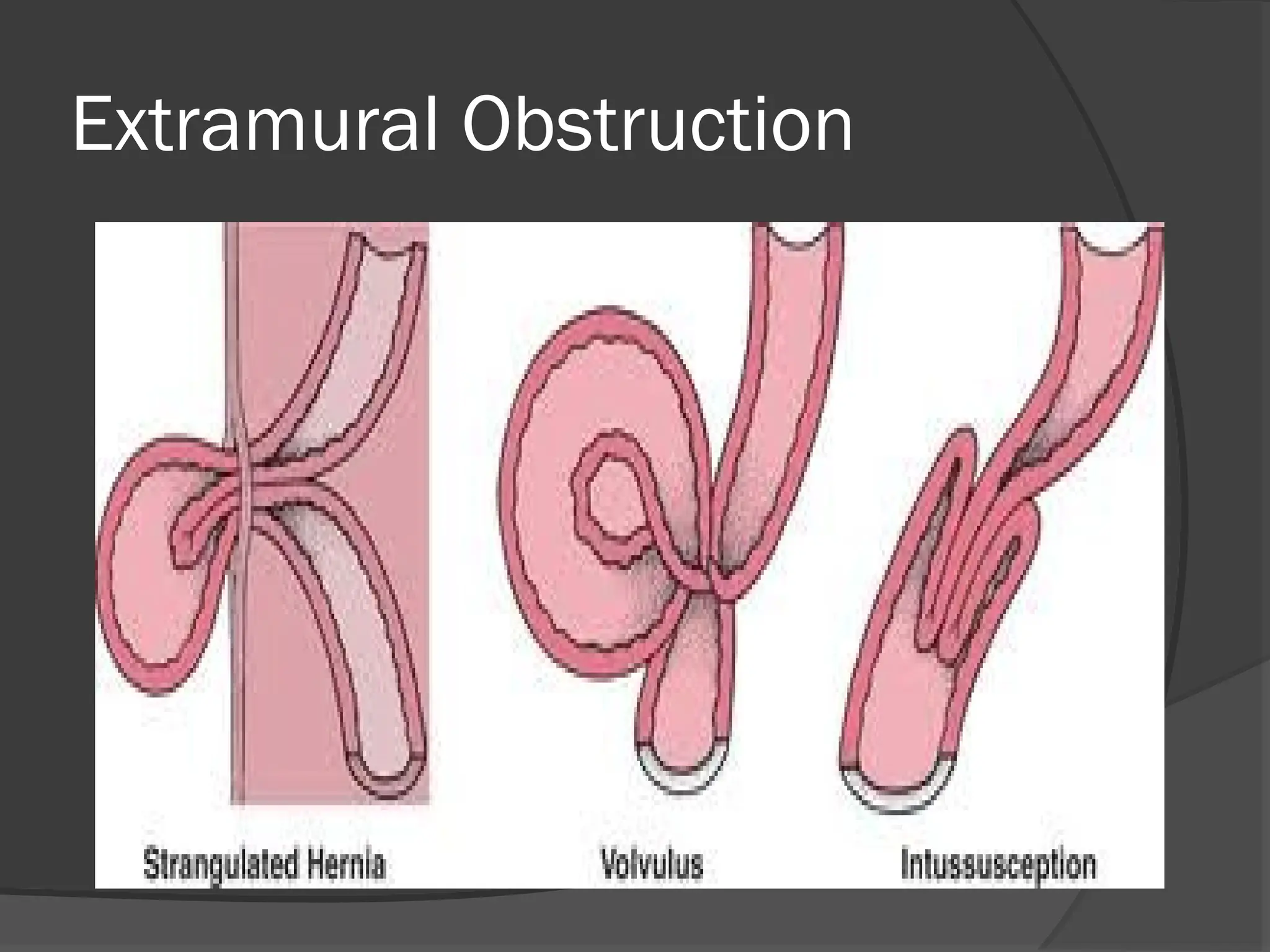
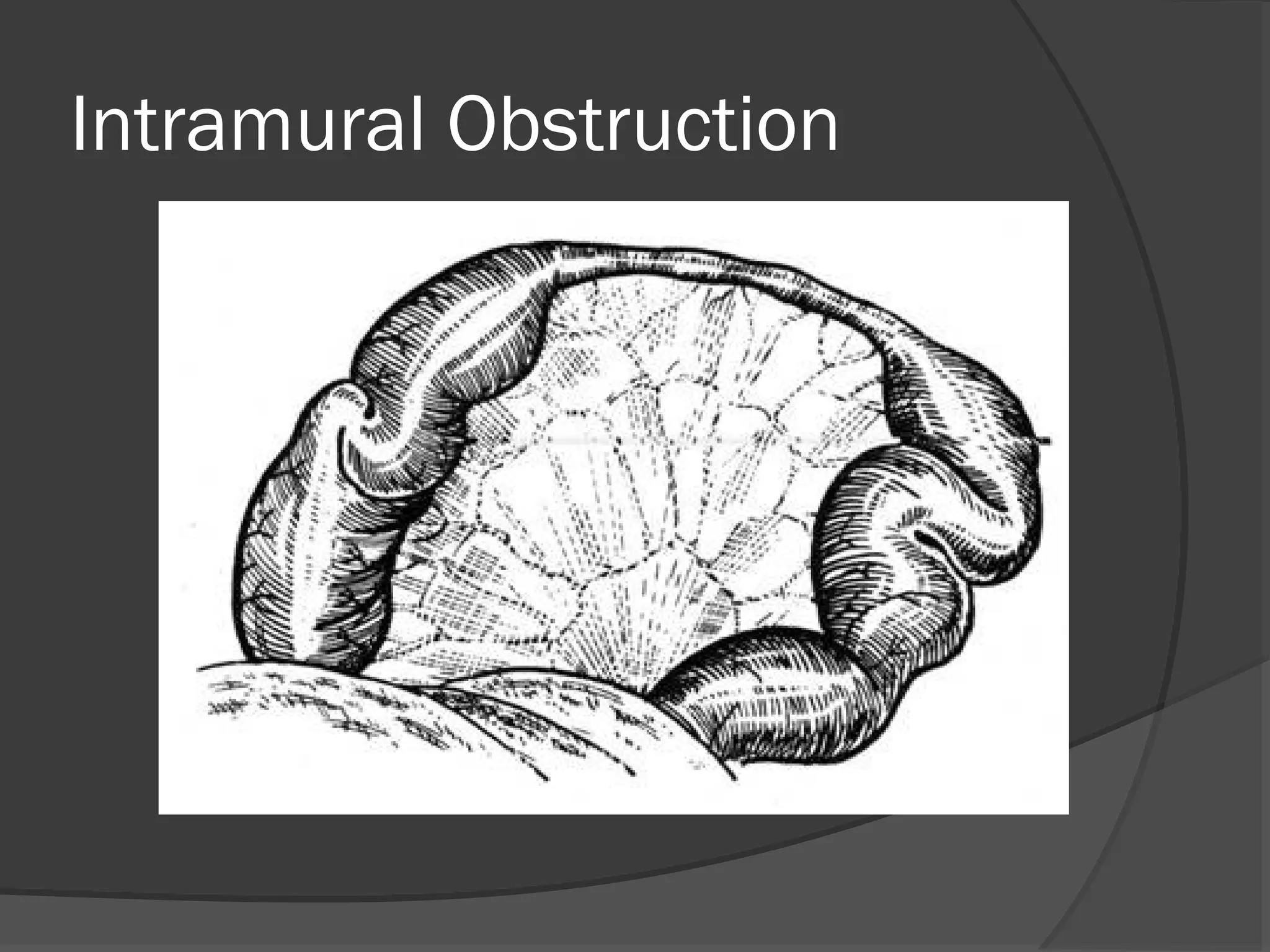
The obstructing lesion may be:
1. Intraluminal (Ex. impacted faeces,
foreign bodies, bezoar, gallstones)
2. Intramural (Ex. malignant or
inflammatory strictures)
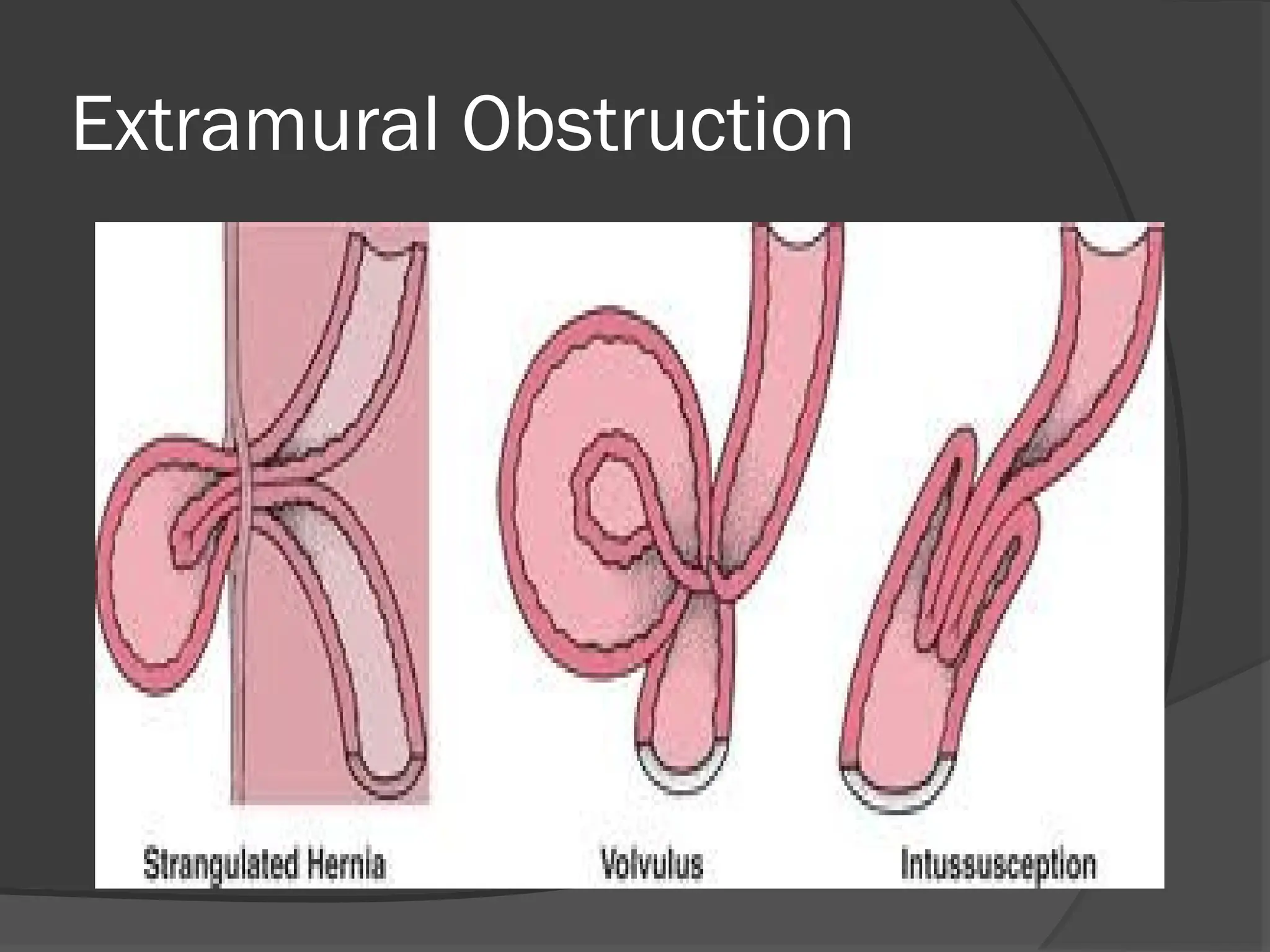
3. Extramural (Ex. intraperitoneal bands
and adhesions, hernias, volvulus or
intussusception.)
Peristalsis is
absent (Ex.
Paralytic ileus) or it
may be present in
a non-propulsive
form (Ex. Pseudo-
obstruction)
Adynamic
Peristalsis maybe absent (e.g. paralytic ileus)
It may be present in a non-propulsive form (e.g.
mesenteric vascular occlusion or
pseudo-obstruction).
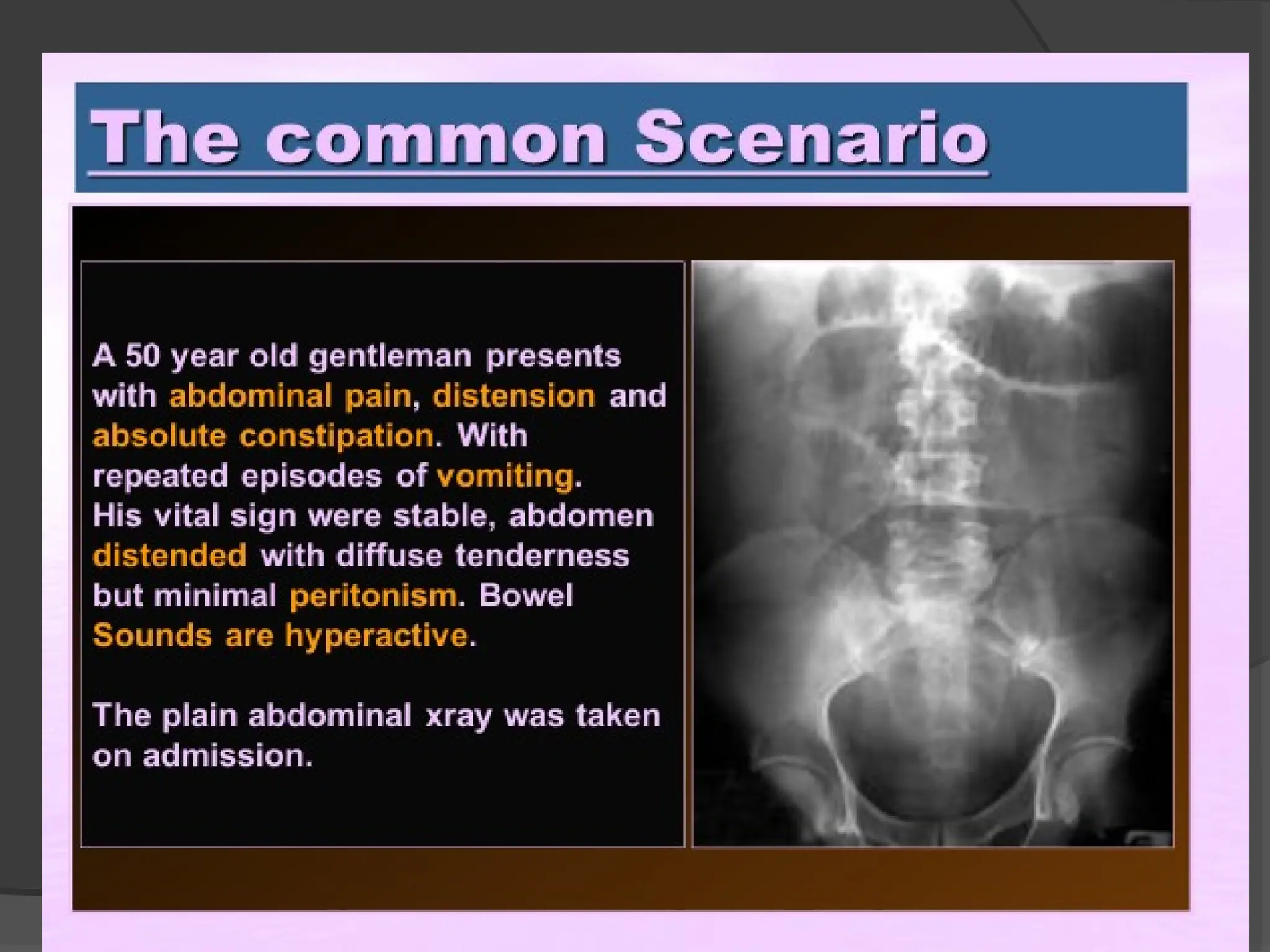
HISTORY - Thediagnosis of intestinal obstruction is based on its “cardinal symptoms”
of Pain, Distension, Vomiting and Absolute Constipation.
Clinical Presentation
1) DURATION - Nature of Presentation of Obstruction will be influenced by
whether the presentation is…
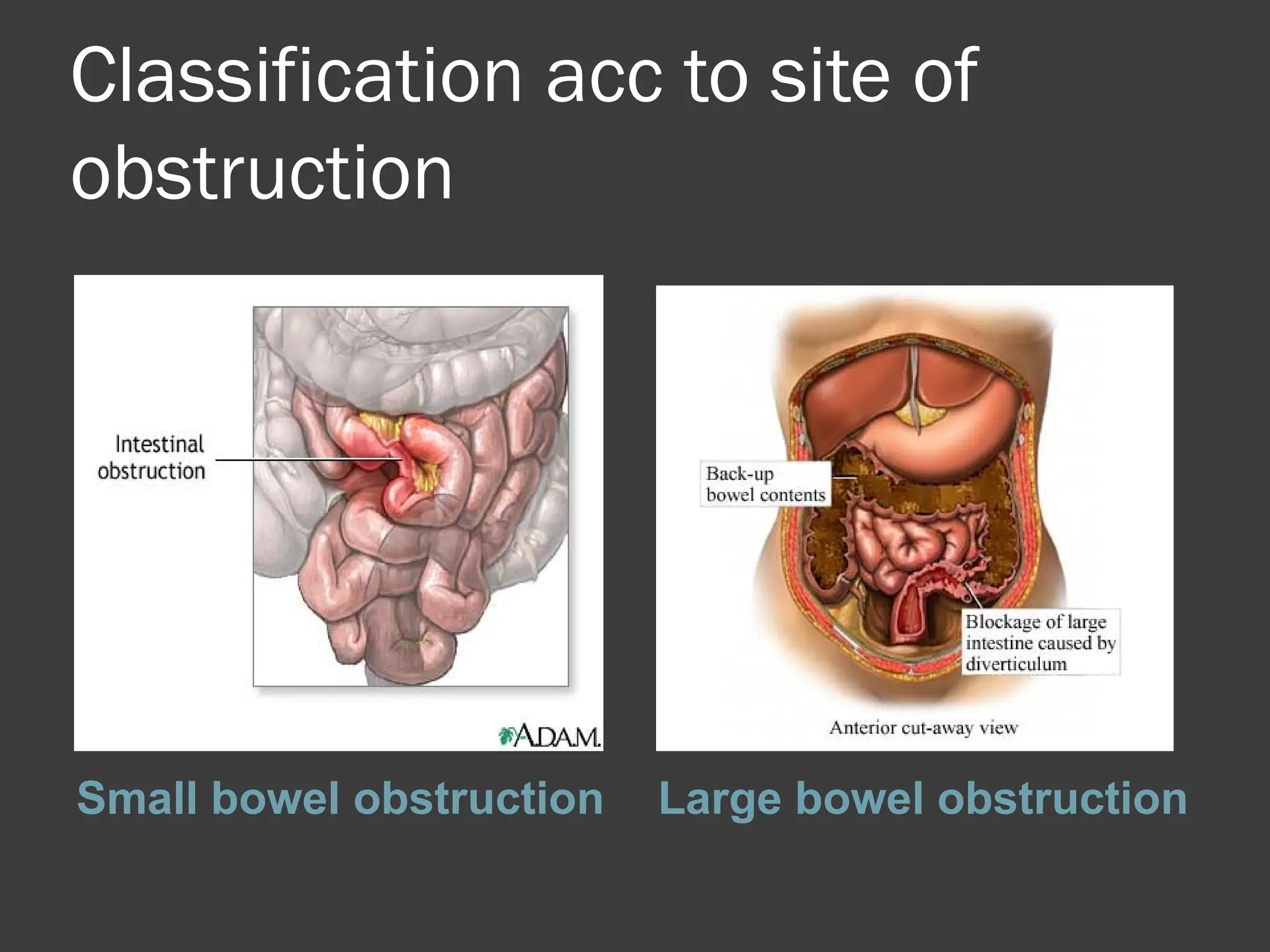
I. Acute Obstruction usually occurs in small bowel obstruction with sudden
onsets of severe colicky central abdominal pain, distension, with early
vomiting and constipation.
II. Chronic obstruction is usually seen in large bowel obstruction with lower
abdominal colic and absolute constipation, followed by distension.
III. In Acute on Chronic Obstruction there is a short history of distention and
vomiting against a background of pain and constipation.
IV. Subacute Obstruction implies an incomplete obstruction. Presentation
will be further influenced by whether the obstruction simple (With blood
supply is intact) or strangulated (there is interference to blood flow)
21.
HISTORY - Thediagnosis of intestinal obstruction is based on its “cardinal symptoms”
of Pain, Distension, Vomiting and Absolute Constipation.
Clinical Presentation
2) PAIN - The Pain of intestinal obstruction is true colic, and it is the first
symptom encountered.
Site- Centered around the umbilicus (small Bowel Colic)
Lower 1/3 of Abdomen (Large Bowel Colic)
Onsite- Sudden
Character - Colicky i.e. pain caused by spasm, intermittent.
Radiation - No Radiation. Generally Periumbilical or Suprapubic.
Associated Symptoms- None.
Timing- Small Bowel colic occurs every 2-20 minutes.
Large Bowel Colic occurs about every 30 minutes or more.
Exacerbating and Relieving Factors- Corresponds with Peristalsis
Severity- Sever.
22.
HISTORY - Thediagnosis of intestinal obstruction is based on its “cardinal symptoms”
of Pain, Distension, Vomiting and Absolute Constipation.
Clinical Presentation
3)VOMITING - Frequent vomiting, nature of Vomitus
depends on the level of obstruction.
I. Pyloric Obstruction vomitus is watery and acidic.
II. High Small Bowel Obstruction vomitus is
Greenish-Blue and Bile-Stained.
III. Lower Small Bowel Obstruction vomitus is foul
smelling and Brown (Faeculent Vomit)
IV. Large Bowel Obstruction vomitus is usually a late
symptom.
23.
HISTORY - Thediagnosis of intestinal obstruction is based on its “cardinal symptoms”
of Pain, Distension, Vomiting and Absolute Constipation.
Clinical Presentation
4) DISTENTION - The lower the site of obstruction
the more bowel there is available to distend.
“Higher up” Bowel Obstruction is NOT
associated with distension.
“Colon” Obstruction causes the colon to
distend around the periphery of the abdomen
and might extend into the small bowel if the
ileocaecal valve is incompetent.
24.
HISTORY - Thediagnosis of intestinal obstruction is based on its “cardinal symptoms”
of Pain, Distension, Vomiting and Absolute Constipation.
Clinical Presentation
5) ABSOLUTE CONSTIPATION - Develops
once the block becomes complete and the
bowel below is empty, so that neither feces
nor flatus are passed.
Occurs Early in “lower” Large Bowel
Obstruction.
Occurs Late in “High” Small Bowel
Obstruction.
25.
HISTORY - Thediagnosis of intestinal obstruction is based on its “cardinal symptoms”
of Pain, Distension, Vomiting and Absolute Constipation.
Clinical Presentation
7) Late Manifestations…
Pyrexia
Respiratory Distress
Dehydration
Hypovolemic Shock
Peritonism
EXAMINATION
Clinical Presentation
4) AUSCULTATION– Bowel Sounds are
Initially Loud and frequent→ Then as
bowel distends the sounds become more
resonant and high pitched→ Eventually
becoming Amphoric.
→
Radiological diagnosis
Radiological diagnosisis based on a supine
abdominal film
Obstructed small bowel -straight segments
that are generally central and lie
transversely. No gas is seen in the colon.
Jejunum -valvulae conniventes
37.
Ileum -featureless
Caecum-a rounded gas shadow in the right iliac
fossa.
Large bowel- haustral folds
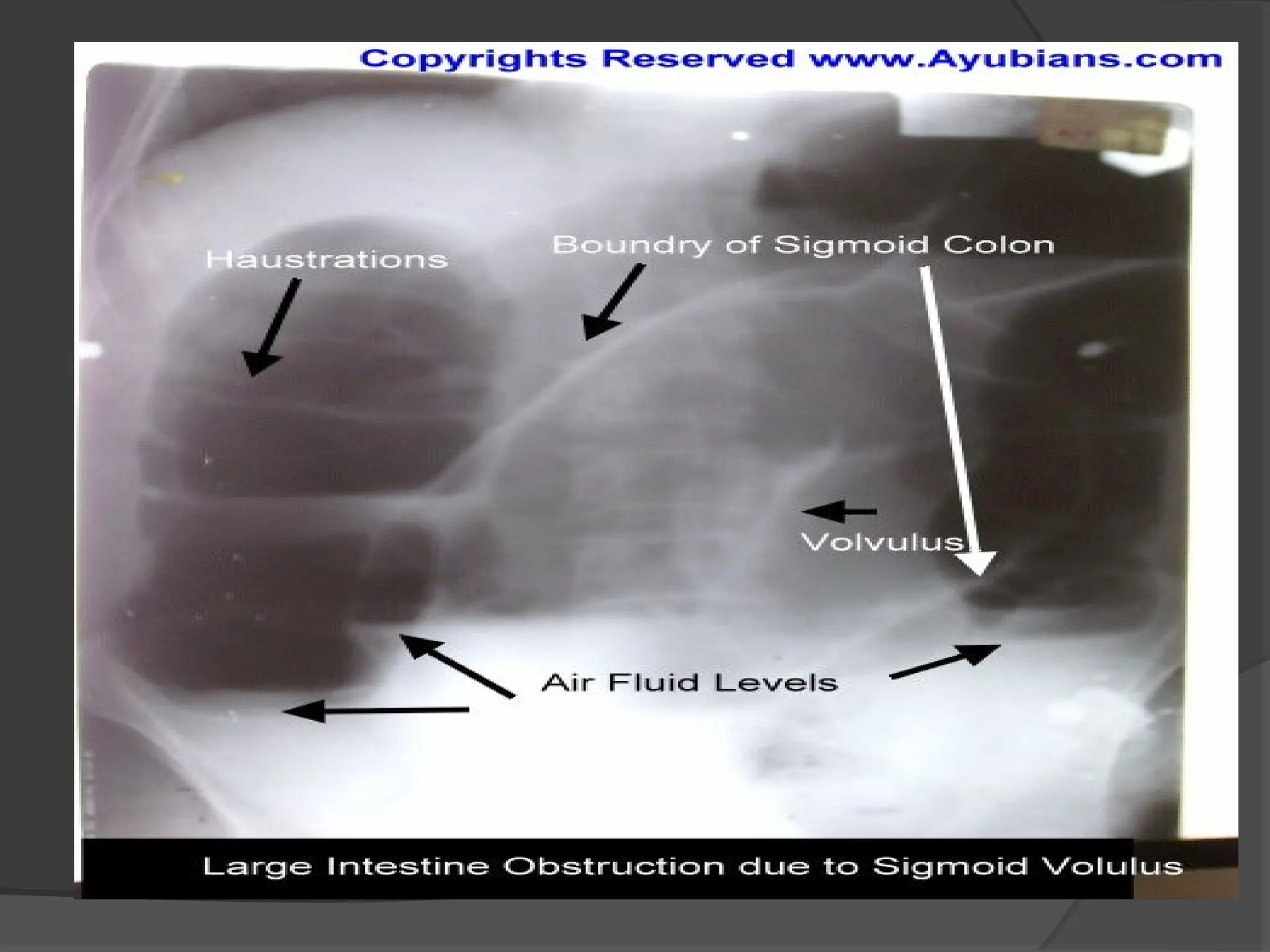
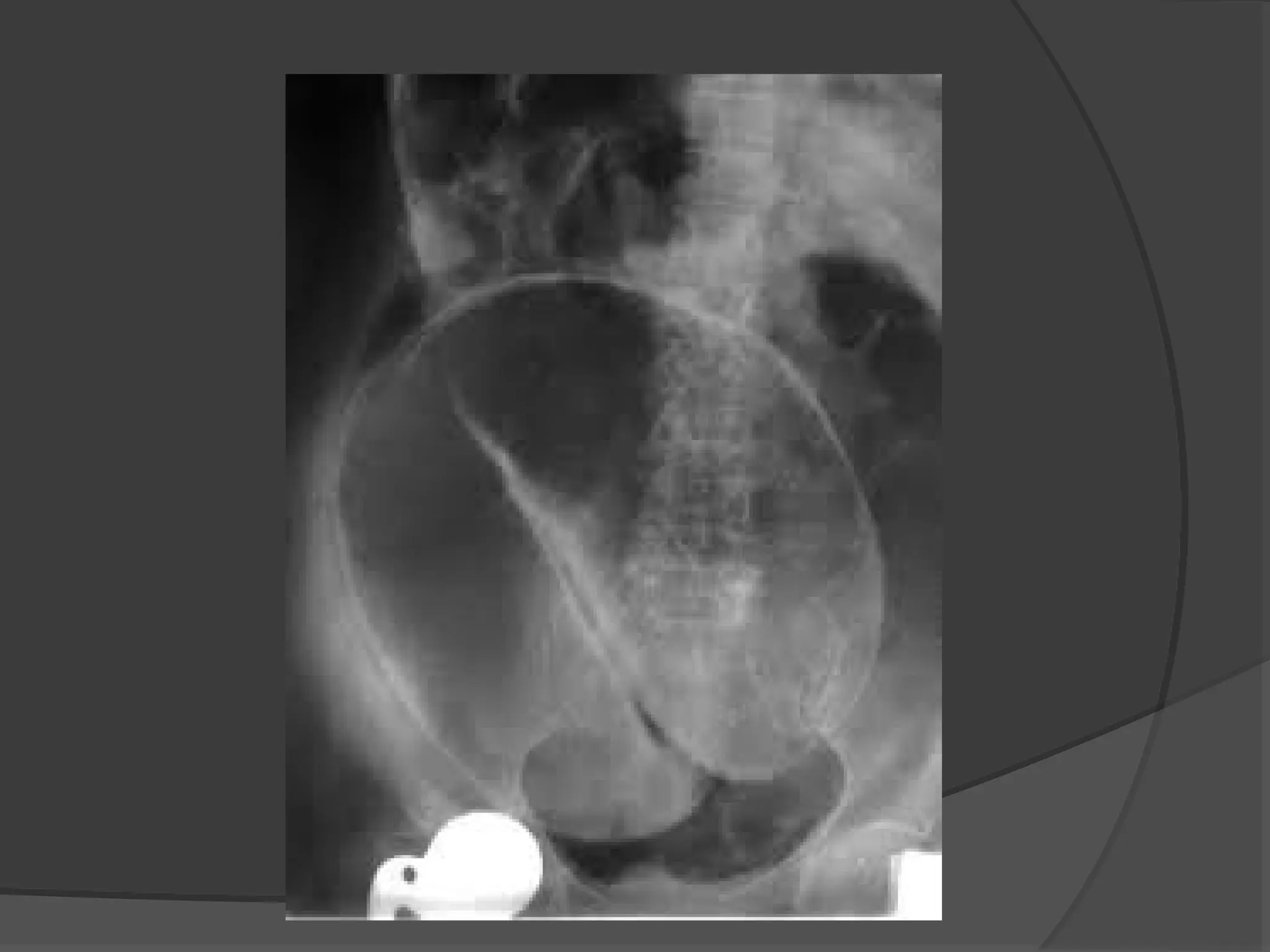
Volvulus of the sigmoid colon -a grossly dilated
loop of colon, with or without visible haustrae
which arises from the pelvis and extends
obliquely across the spine to the upper abdomen.
38.
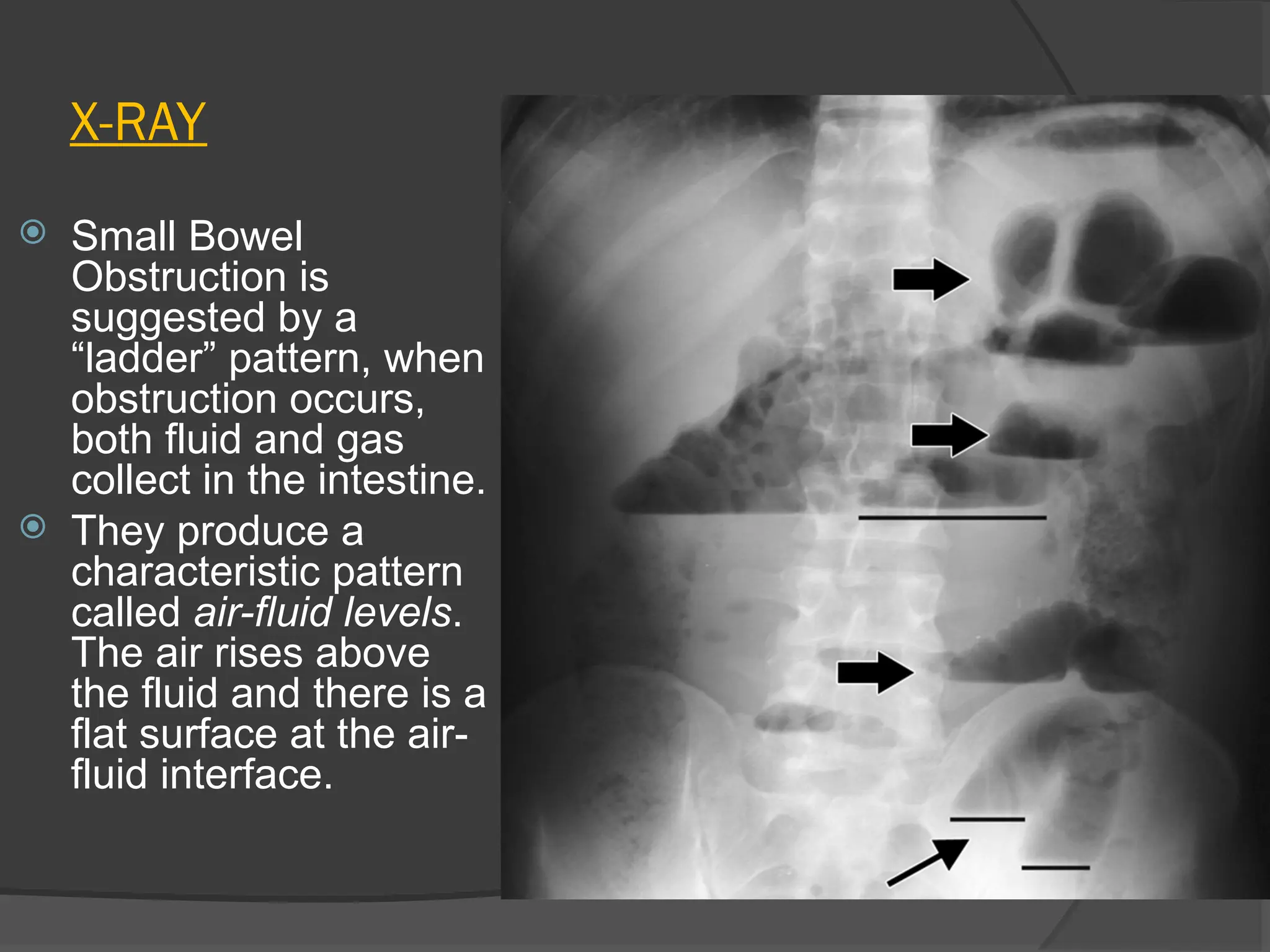
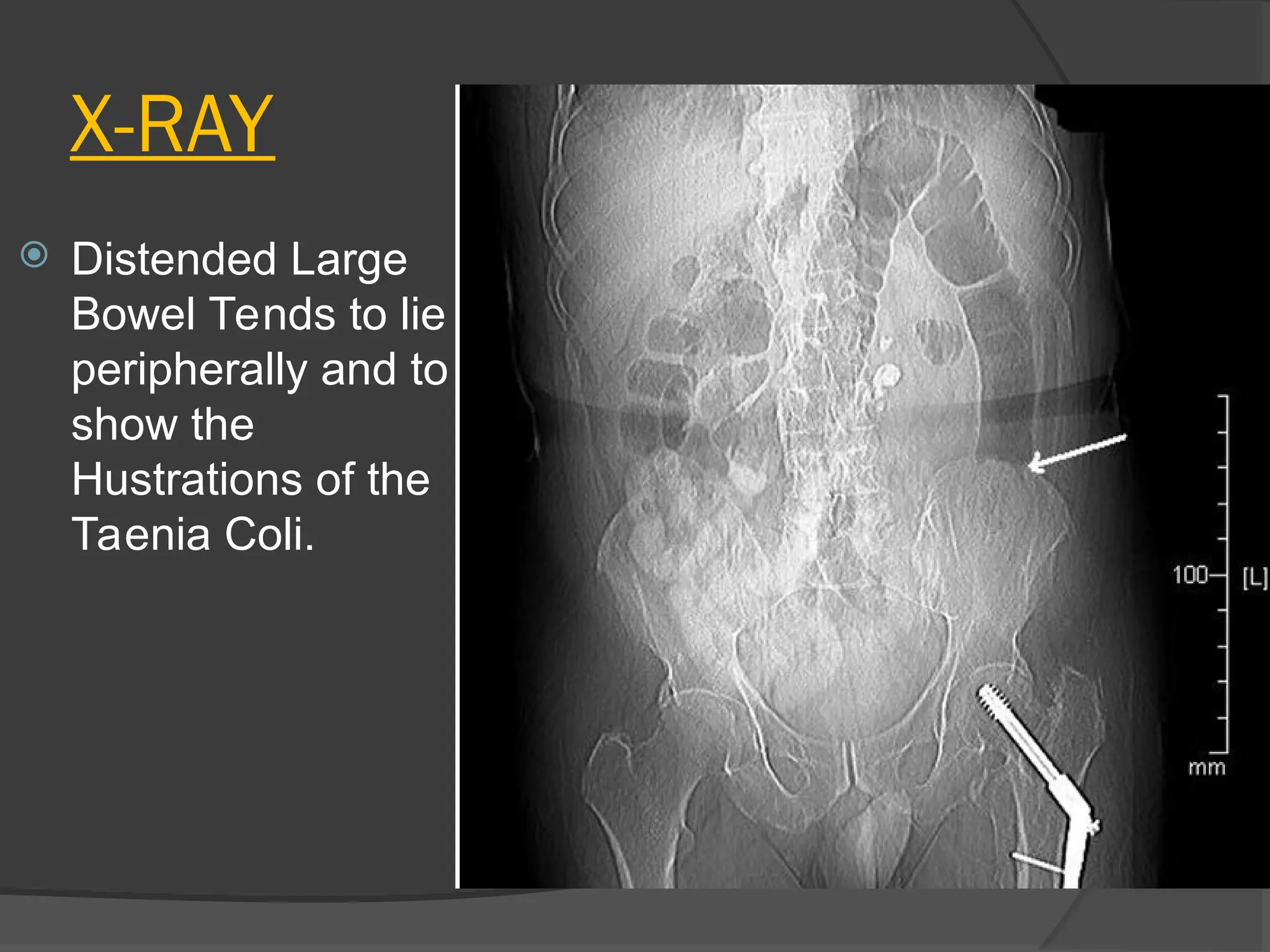
X-RAY
Small Bowel
Obstructionis
suggested by a
“ladder” pattern, when
obstruction occurs,
both fluid and gas
collect in the intestine.
They produce a
characteristic pattern
called air-fluid levels.
The air rises above
the fluid and there is a
flat surface at the air-
fluid interface.
X-RAY- “Barium Follow-Through”
Patient drinks a contrast medium containing
barium sulfate. Contrast medium appears
white on x-rays, and shows the outline of the
internal lining of the bowel.
X-ray images are taken at intervals as the
contrast moves through the intestine, (@ 0
minutes→@ 20 minutes→@ 40 minutes →
@90 minutes);
The bowel is accessed as it becomes visible.
The test is completed when the Barium is
visualized at the Caecum.
Although the treatmentof
specific causes of intestinal
obstruction is considered
accordingly, there are some
general principles applied.
Chronic large bowel
obstruction, slowly progressive,
and incomplete obstruction can
be investigated at some leisure.
Acute, sudden onset, complete
and obstruction with risk of
strangulation requires emergency
surgical intervention.
48.
Treatment of acuteintestinal
obstruction
Principles of treatment
Gastrointestinal drainage
Fluid and electrolyte replacement
Relief of obstruction, usually surgical
49.
Preop
1. Gastric Aspirationvia Nasogastric Tube; This
decompress the bowel and remove risk of
inhaling gastric contents during anesthesia.
2. IV Fluid replacement Give normal Saline,
Possibly Blood or Plasma if patient is shocked.
1. Antibiotic Therapy Started if Strangulation is
found or suspected.
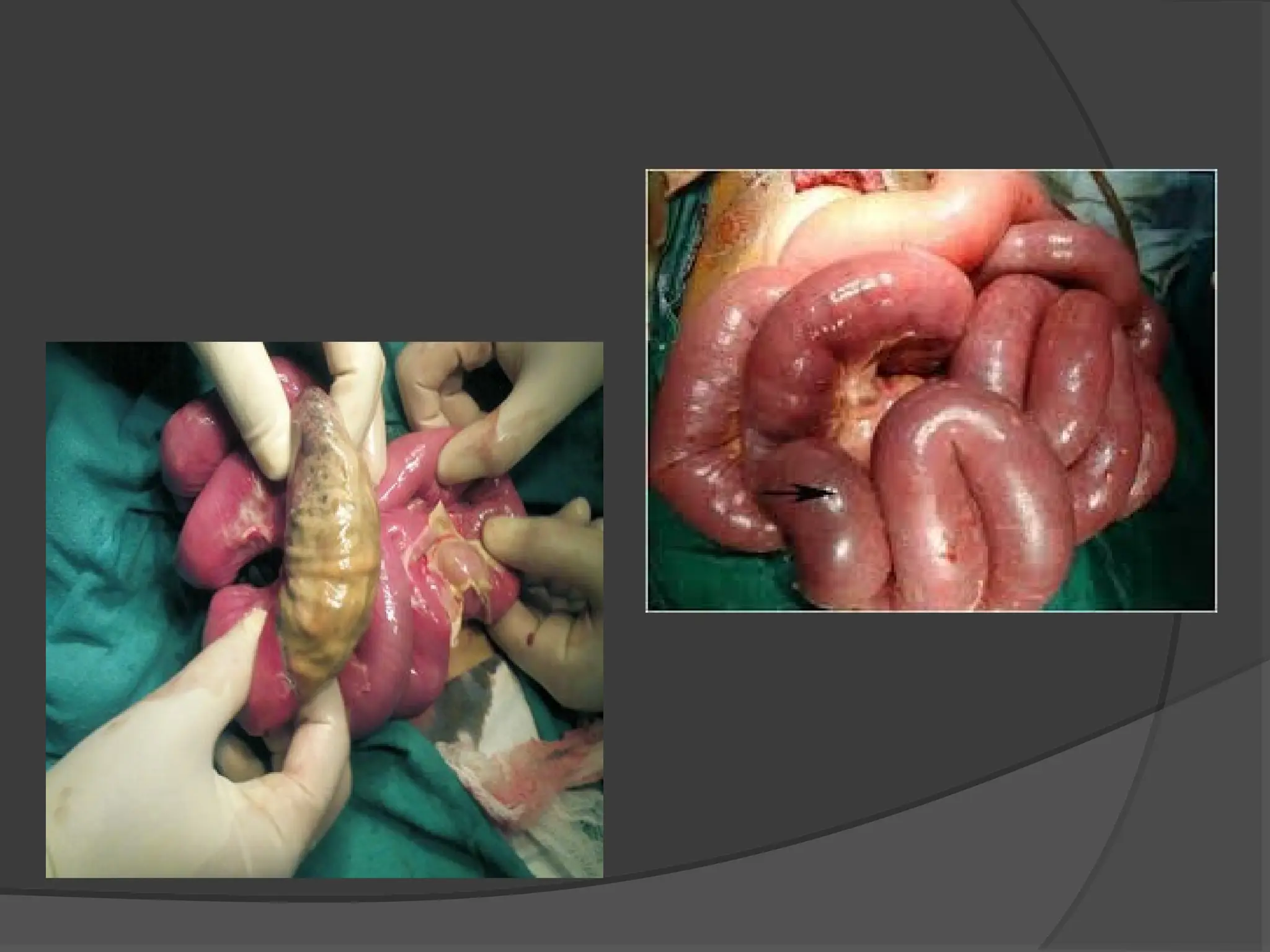
Bowel isinspected and
non-viable (aka non-
functioning) bowel is
removed.
Non-Viability is determined by:
I. Loss of peristalsis
II. Loss of Sheen
III. Greenish or Black (Not
Purple; Purple may still
recover)
IV. Loss of Pulsation in
supplying vessels
Small Bowel can be
removed and anastomosis
performed with safety
because of its rich blood
supply.
Large bowel is not as
easily approachable,
where consideration must
be taken regarding the
location of the obstruction
and its relation to nearby
blood supply.
Operative
54.
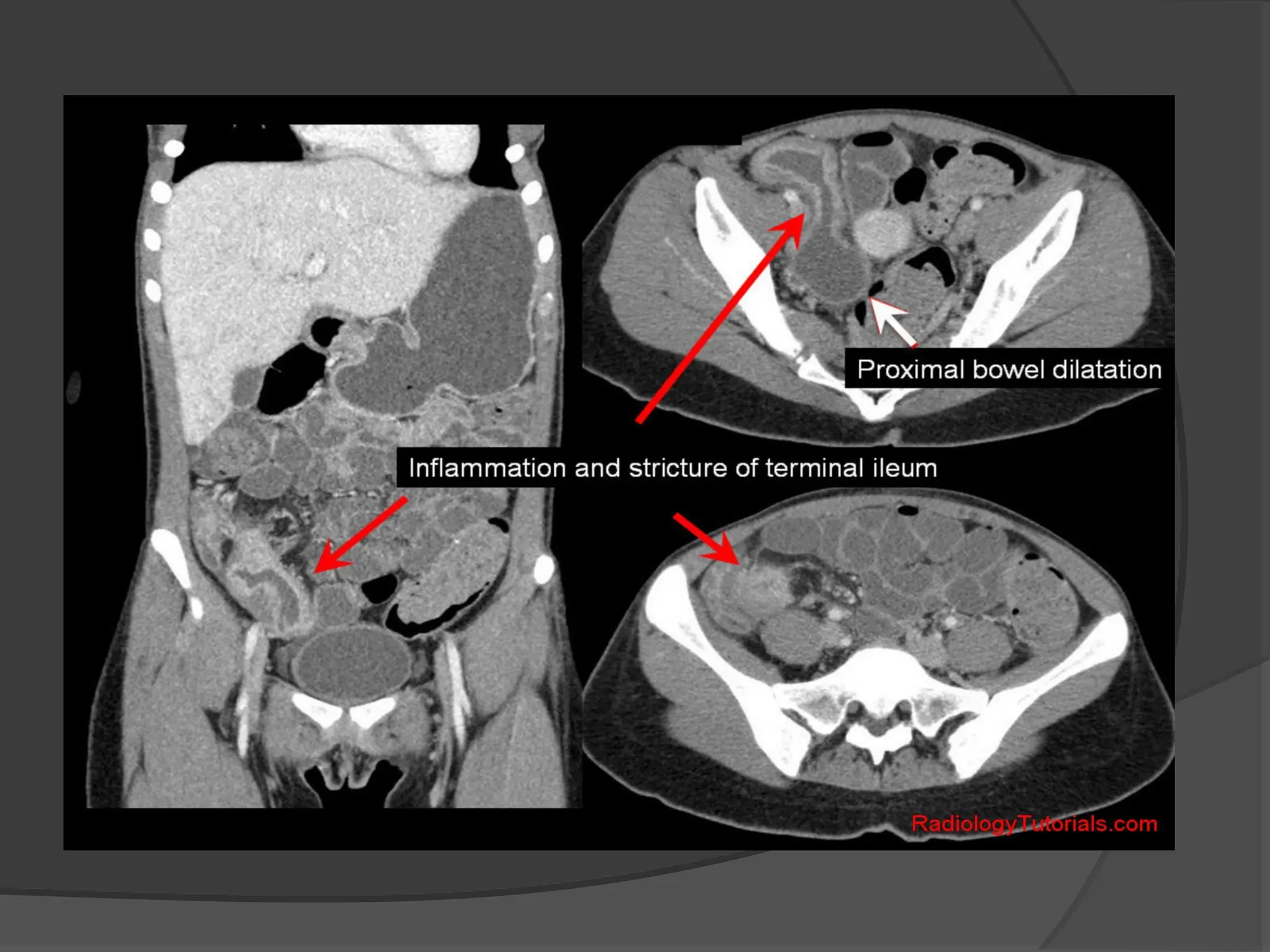
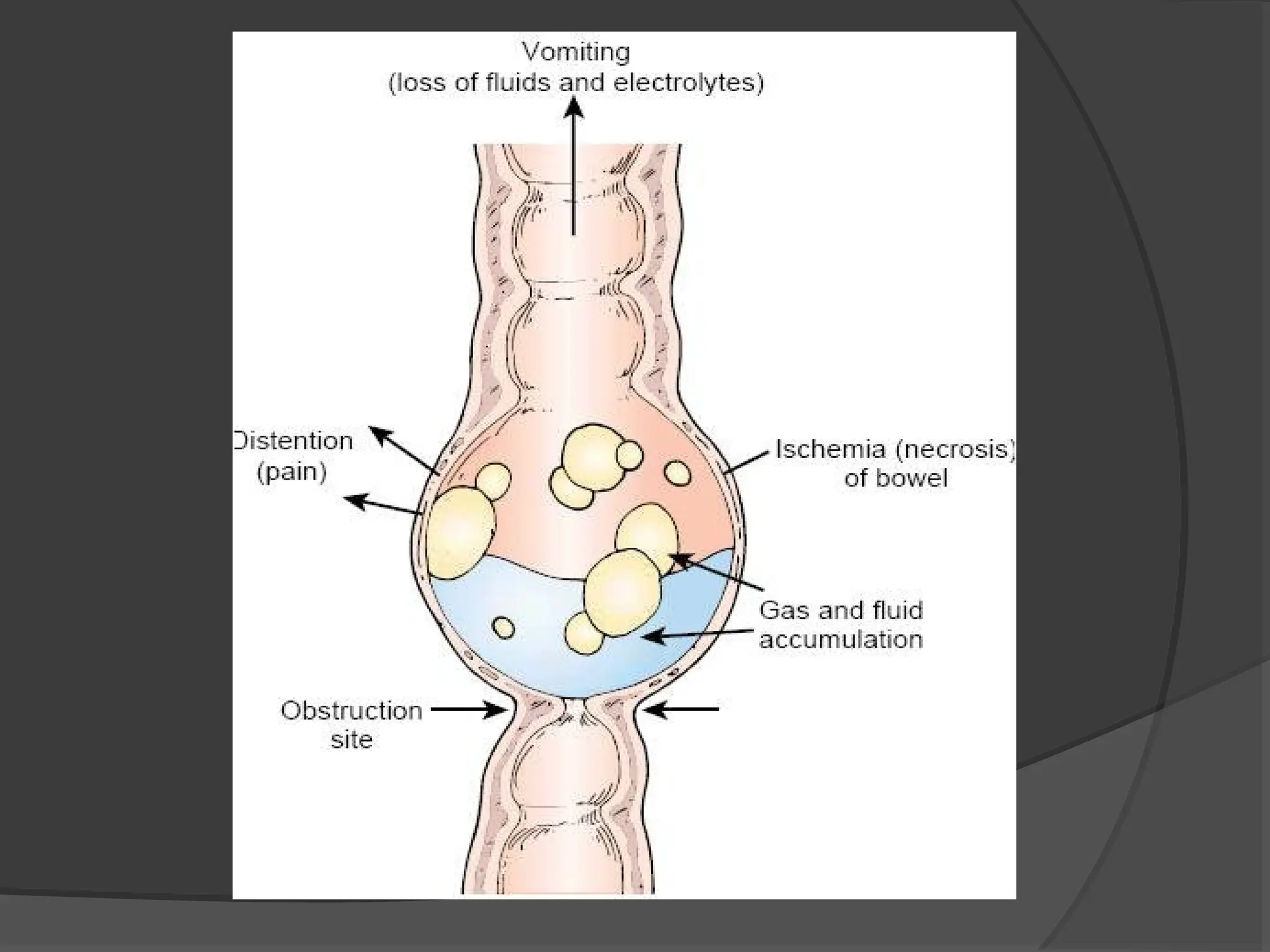
Pathophysiology
In obstruction,regardless of the cause of obstruction
or its acuteness of onset, the proximal bowel dilates
and develops an altered motility.
Below the obstruction, the bowel exhibits normal
peristalsis and absorption until it becomes empty,
when it contracts and becomes immobile.
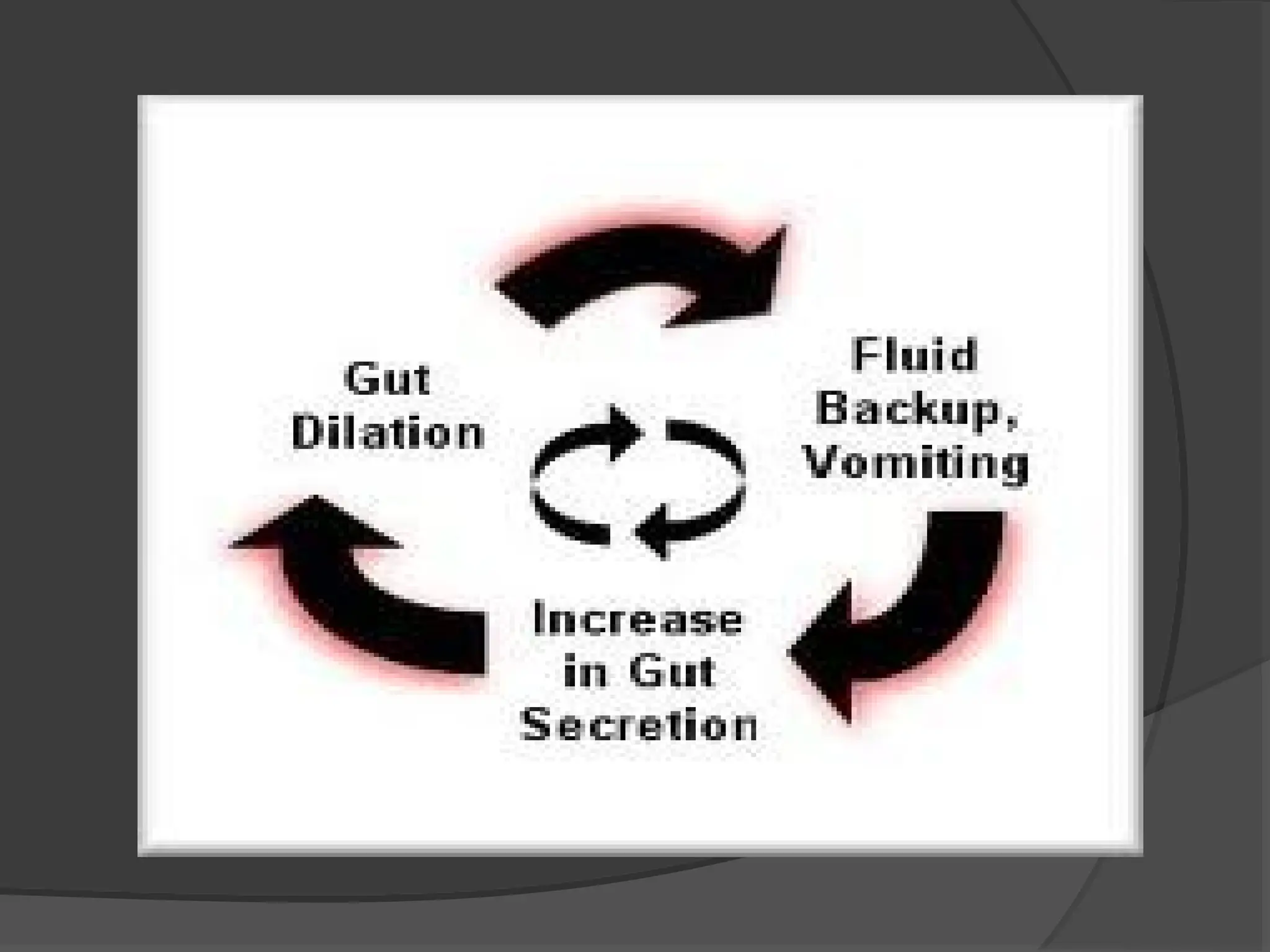
Initially, proximal peristalsis is increased to
overcome the obstruction, If the obstruction is not
relieved the bowel begins to dilate causing a
reduction in peristaltic strength, ultimately resulting
in flaccidity and paralysis.
58.
The distensionproximal to an obstruction
is produced by two factors:
I. Gas
II. Fluid
62.
Strangulation
Strangulation
Strangulation is verydangerous condition and
Strangulation is very dangerous condition and
demands early treatment before gangrene of the
demands early treatment before gangrene of the
bowel arises
bowel arises
.
.
62
62
63.
Strangulation
Strangulation isimpairment of blood supply to bowel.
Signs of Strangulation
• Toxic Appearance, Rapid Pulse, Temperature drop
• Colicky pain with decreasing intermittence
• Marked Tenderness and Rigidity
• Raised WBC (mainly Neutrophils), usual with
infracted bowel.
• Shock
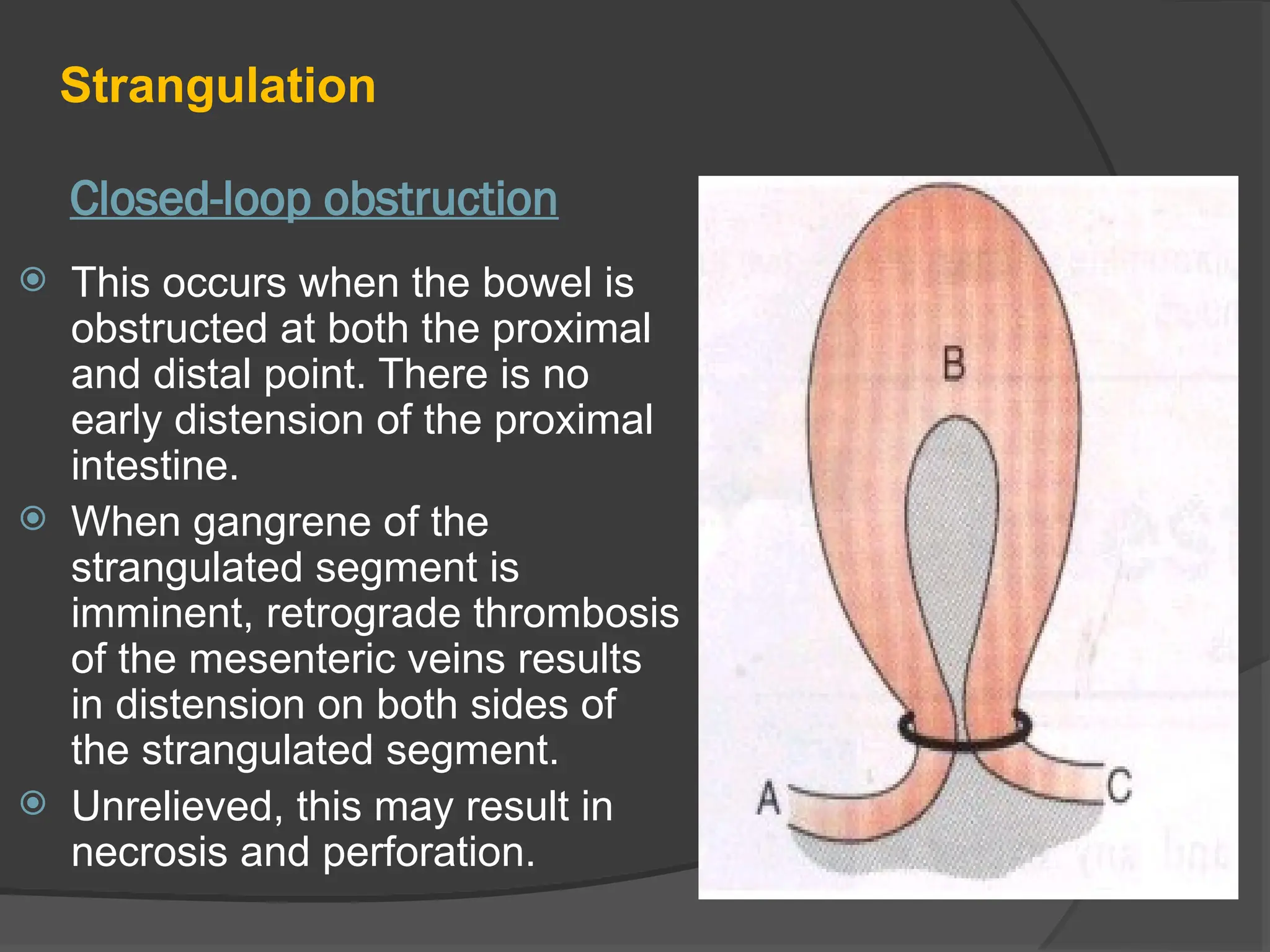
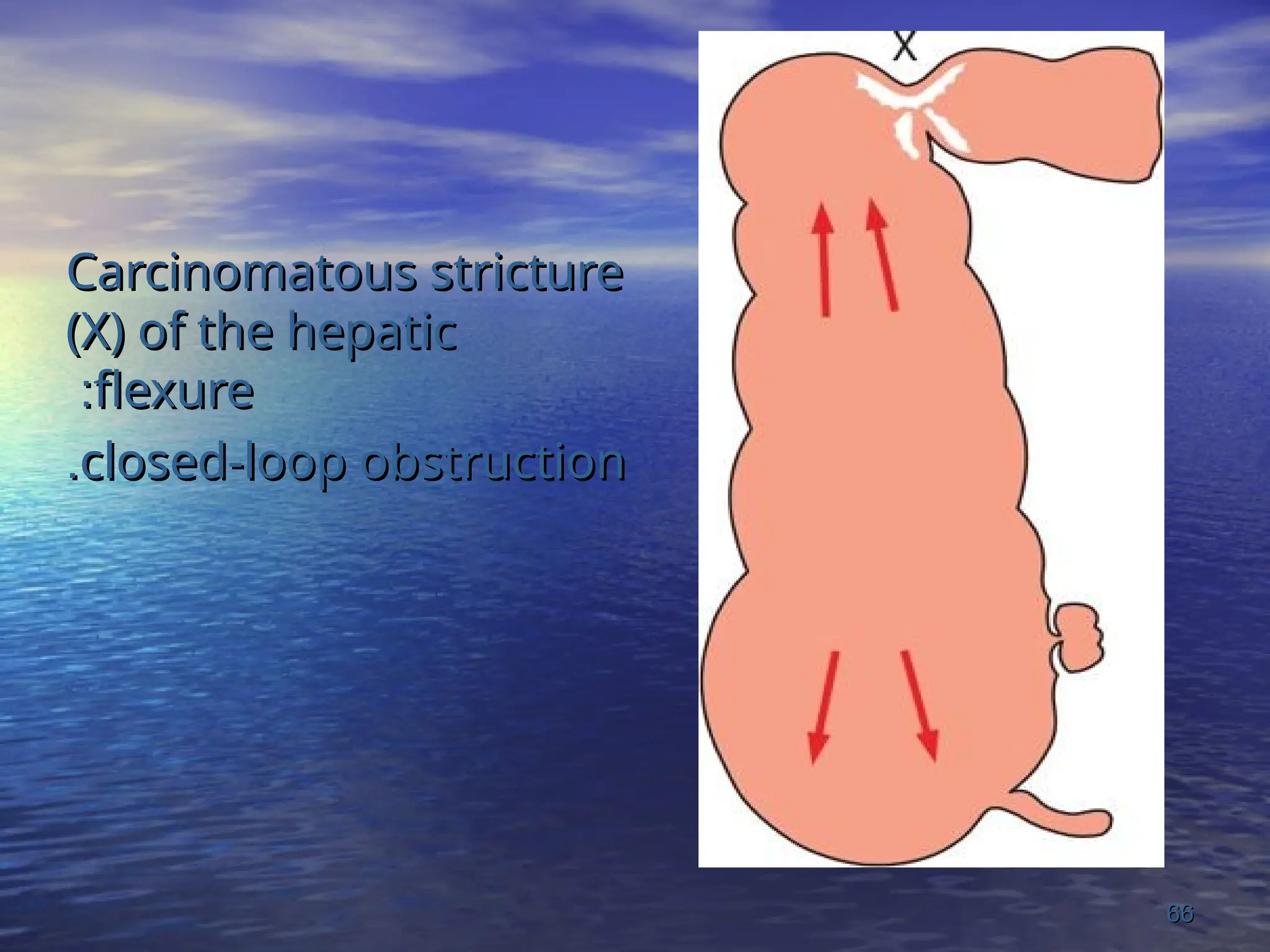
Closed-loop obstruction
Strangulation
Thisoccurs when the bowel is
obstructed at both the proximal
and distal point. There is no
early distension of the proximal
intestine.
When gangrene of the
strangulated segment is
imminent, retrograde thrombosis
of the mesenteric veins results
in distension on both sides of
the strangulated segment.
Unrelieved, this may result in
necrosis and perforation.
Internal Hernia
Internal Hernia
:
:
Thefollowing are potential sites of internal
The following are potential sites of internal
herniation (all are rare)
herniation (all are rare)
:
:
1
1
-
-
The foramen of winslow
The foramen of winslow
.
.
2
2
-
-
A hole in the mesentery
A hole in the mesentery
.
.
3
3
-
-
A defect in the transverse mescolon
A defect in the transverse mescolon
.
.
4
4
-
-
Defects in the broad ligament
Defects in the broad ligament
.
.
5
5
-
-
Congenital or acquired diaphragmatic hernia
Congenital or acquired diaphragmatic hernia
.
.
6
6
-
-
Duodenal retroperitoneal fossae
Duodenal retroperitoneal fossae
.
.
7
7
-
-
Caecal/appendiceal retroperitoneal fossae
Caecal/appendiceal retroperitoneal fossae
.
.
8
8
-
-
Intersigmoid fossa
Intersigmoid fossa
.
.
67
67
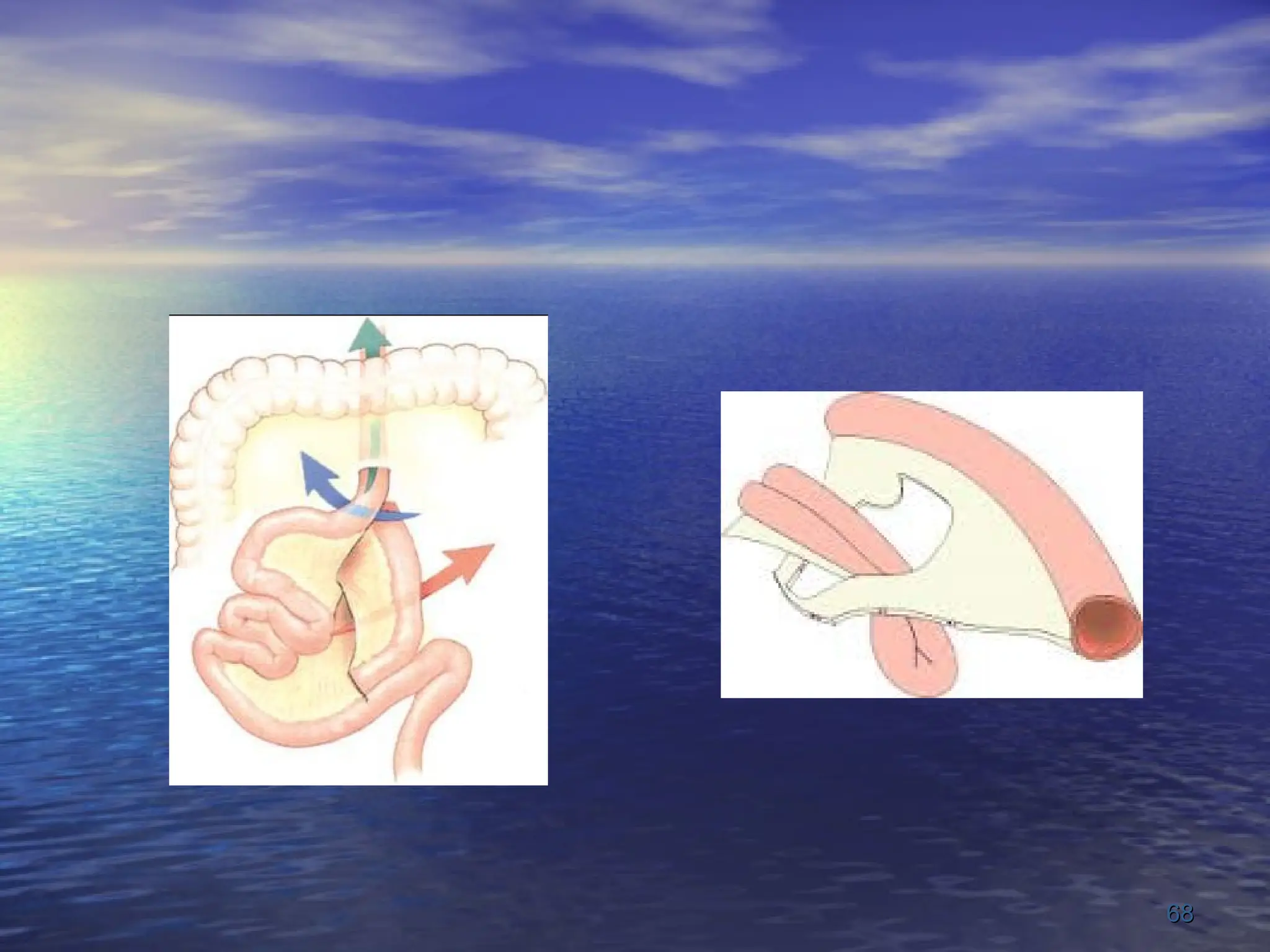
The standard treatmentof an obstructed hernia is
The standard treatment of an obstructed hernia is
to release the constricting agent by division
to release the constricting agent by division
.
.
This should not be undertaken in cases of
This should not be undertaken in cases of
herniation involving
herniation involving
:
:
Foramen of Winslow
Foramen of Winslow
,
,
Mesenteric defects
Mesenteric defects
Paraduodenal/duodenojejunal fossae
Paraduodenal/duodenojejunal fossae
as major BV run in the edge of the constriction ring
as major BV run in the edge of the constriction ring
.
.
The distended loop in such circumstances must first
The distended loop in such circumstances must first
be decompressed (minimising contamination)
be decompressed (minimising contamination)
and then reduced
and then reduced
.
.
69
69
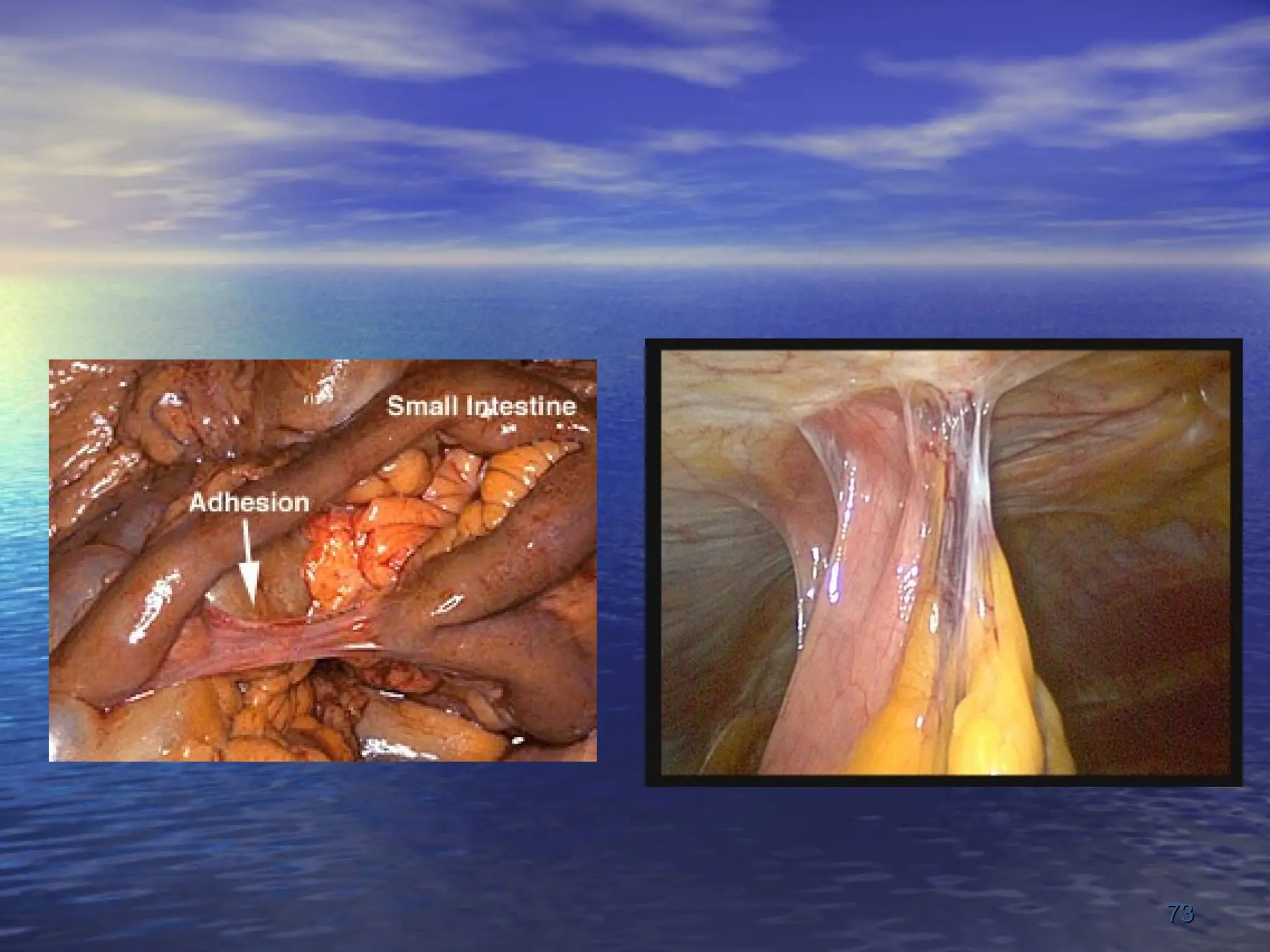
Adhesions
Most commoncause of obstruction in the west.
Any site of peritoneal irritation results in fibrin
production, which results in adhesions between
apposed surfaces.
Only ONE adhesion may be causative of
obstruction.
There are many causes of intraperitoneal
adhesions such as Ischemic Areas, Foreign
Material, Infection, Inflammatory Conditions, and
Radiation Enteritis.
72.
Adhesions
Adhesions mayhe classified into various types
whether they are early (fibrinous), late (fibrous) or
by the underlying etiology. From a practical
perspective, there are only two types — ‘easy’
weak ones and ‘difficult’ dense ones.
Postoperative adhesions giving rise to intestinal
obstruction usually involve the lower small bowel.
Operations for appendicitis and gynecological
procedures are the most common; and are an
indication for early intervention.
**
**
Bands
Bands
:
:
Usually only oneband is culpable, this may be
Usually only one band is culpable, this may be
:
:
1
1
-
-
Congenital: - e.g. obliterated vitellointestinal
Congenital: - e.g. obliterated vitellointestinal
tract
tract
.
.
2
2
-
-
String band following previous bacterial
String band following previous bacterial
peritonitis
peritonitis
.
.
3
3
-
-
Portion of greater omentum usually adherent
Portion of greater omentum usually adherent
to the parietes
to the parietes
.
.
75
75
76.
The followingfactors may limit adhesion formation:
I. Good surgical technique
II. Washing of the peritoneal cavity with saline to remove clots, etc.
III. Minimize contact with gauze
IV. Cover anastomosis and raw peritoneal surfaces.
V. Numerous substances have been instilled in the peritoneal
cavity to prevent adhesion formation, no single agent has been
shown to be safe and effective, and their use is not
recommended.
77.
Treatment
Treatment ofadhesions is initially
Conservative, but should not be prolonged
beyond 72hrs.
In such cases Laparotomy is required, only
causative adhesion should be removed;
removal of other adhesion will only cause
more adhesion formation.
If multiple adhesions must be removed the
bare area should be covered with omental
grafts.
78.
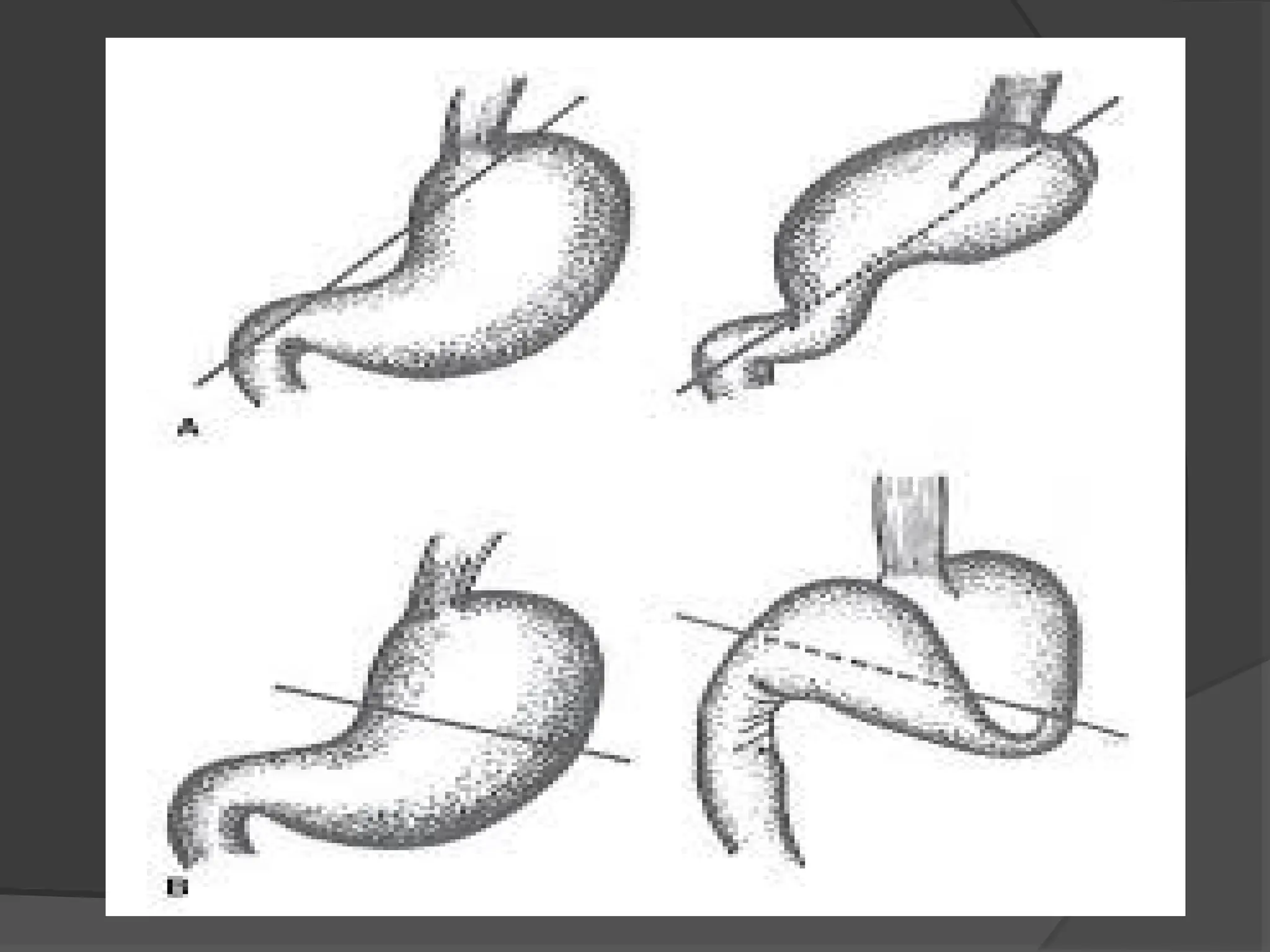
Volvulus
A twistingor axial rotation of a portion of bowel
about its mesentery. When complete it forms a
closed loop of obstruction with resultant ischemia
secondary to vascular occlusion.
May be primary or secondary.
The primary form occurs secondary to congenital
malrotation of the gut, abnormal mesenteric
attachments or congenital bands.
A secondary Volvulus, which is the more common
variety, is due to actual rotation of a piece of bowel
around an acquired adhesion or stoma.
86.
1) Volvulus Neonatorum
Due to arrest gut rotation and narrow
mesentery of small bowel and Caecum .
Symptoms include catastrophic onset of
repeated vomiting, rapid dehydration
and abdominal distension
87.
2) Volvulus ofSmall Intestine
Primary or secondary and usually in
the lower ileum
Spontaneously or secondary
Treatment consists of reduction of the
twist and directed to the underlying
cause .
88.
3) Cecal Volvulus
Primary or as a part of Volvulus Neonatorum .
A clockwise twist ·
F>M .
Acute features of obstruction .
25% has tympanic swelling in the midline or
left side of the abdomen .
89.
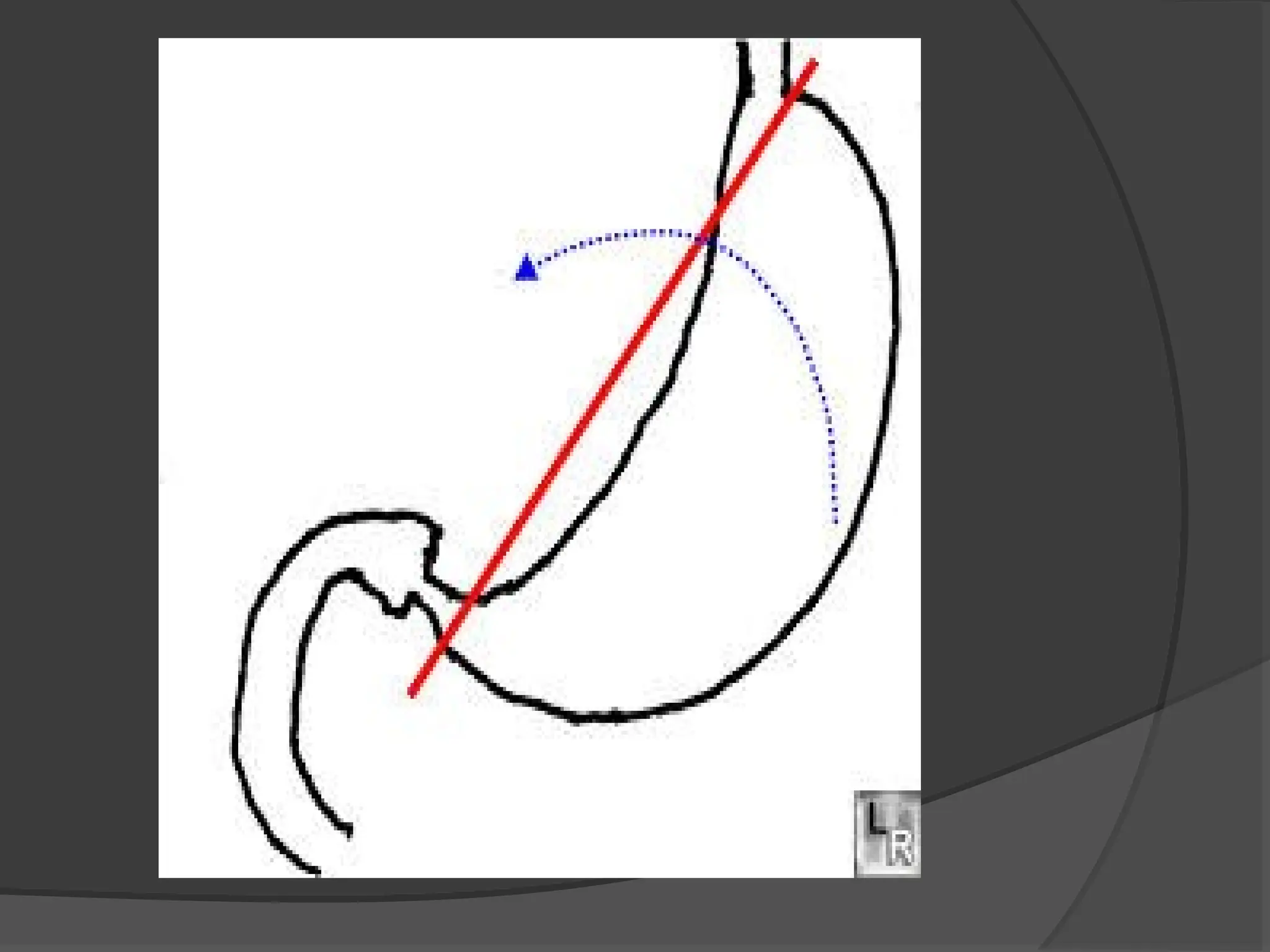
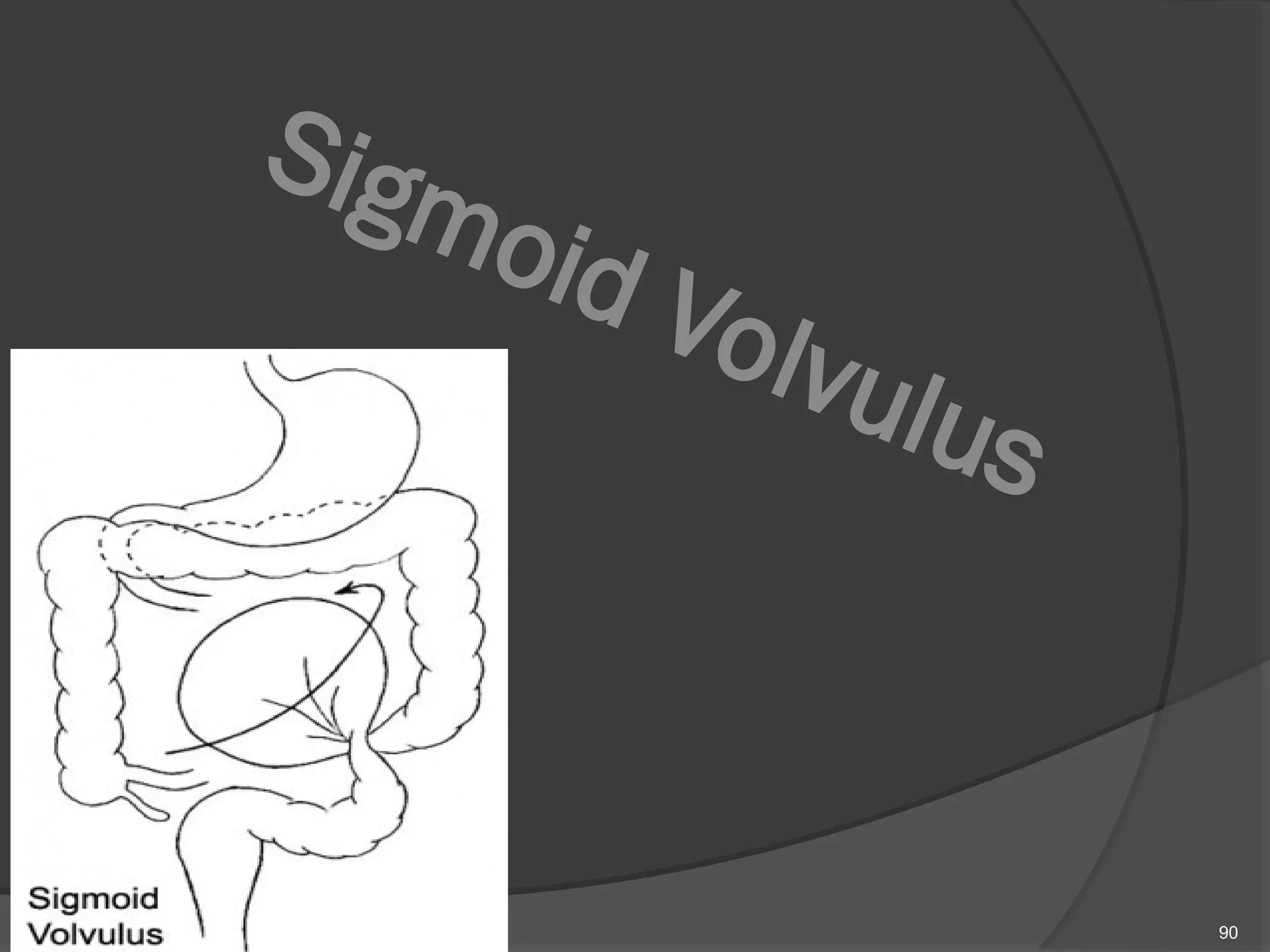
4) Sigmoid Volvulus
An anticlockwise twist .
Most Common spontaneous Volvulus in
Adults.
Chronic constipation is a predisposing
factor.
This is uncommonin Europe and the United States,
but more common in Eastern Europe and Africa.
it is the most common cause of large bowel
obstruction in the Black African population.
Rotation nearly always occurs in the anticlockwise
direction.
91
92.
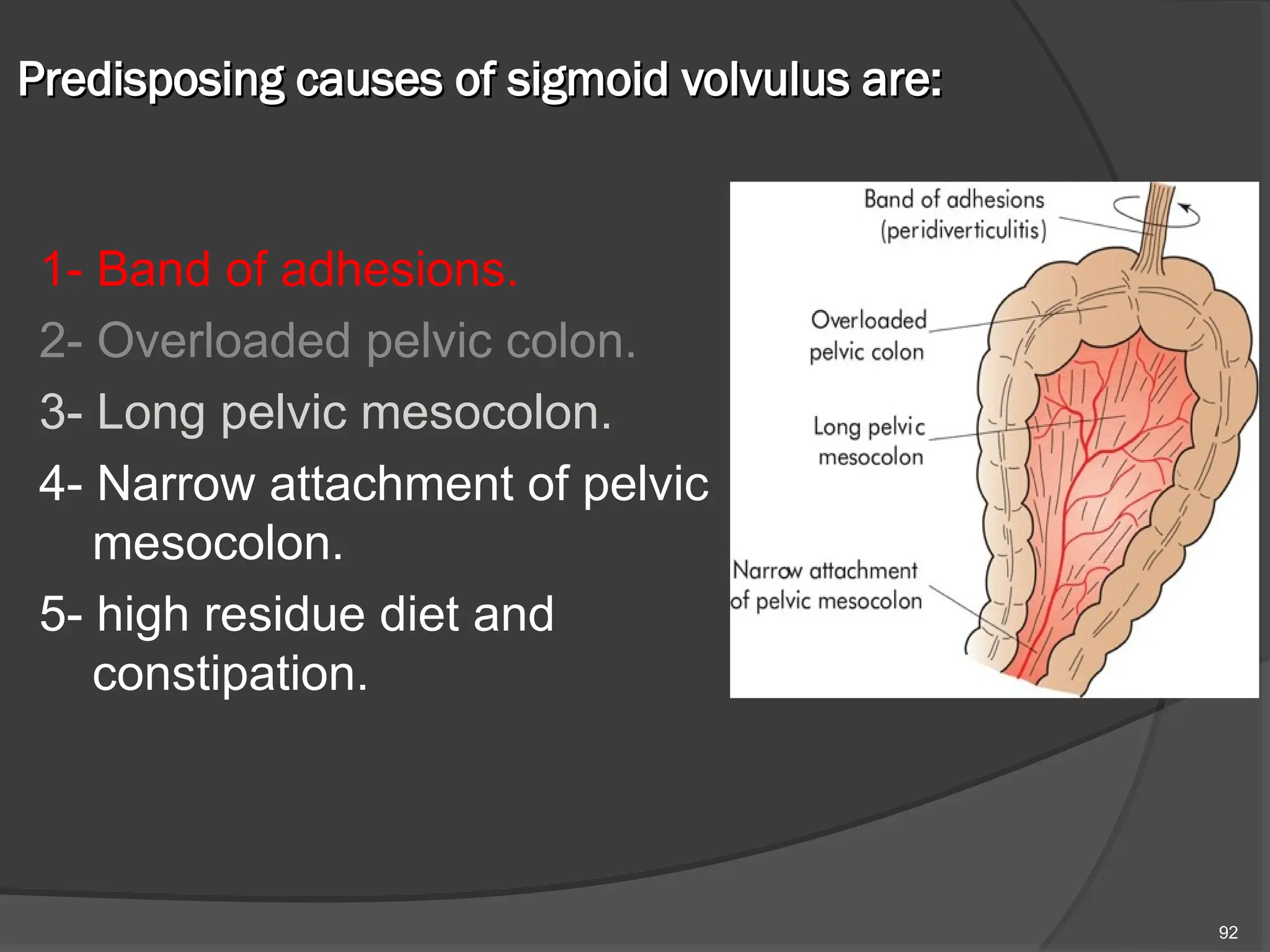
Predisposing causes ofsigmoid volvulus are:
Predisposing causes of sigmoid volvulus are:
1- Band of adhesions.
2- Overloaded pelvic colon.
3- Long pelvic mesocolon.
4- Narrow attachment of pelvic
mesocolon.
5- high residue diet and
constipation.
92
93.
In Western populations,the condition is seen most
often in elderly patients with chronic constipation;
comorbidities are common and chronic psychotropic
drug use is associated with this condition.
Younger patients present earlier and the prognosis is
inversely related to the duration of symptoms.
Presentation can be classified as:
* Fulminant: sudden onset, severe pain, early
vomiting, rapidly deteriorating clinical course;
* Indolent: insidious onset, slow progressive course,
less pain, late vomiting.
93
94.
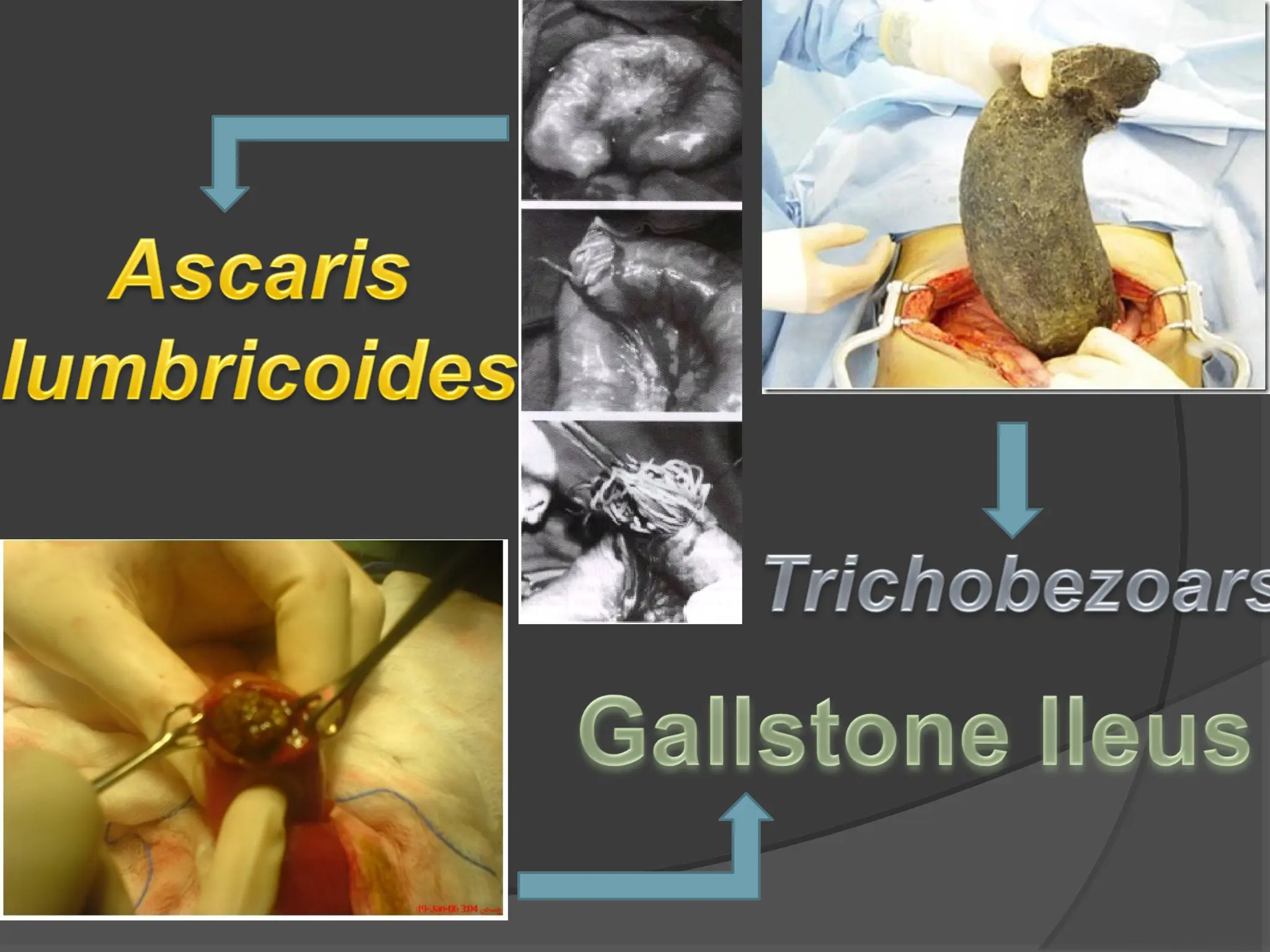
Bolus Obstruction.
“Accumulation →Compaction”
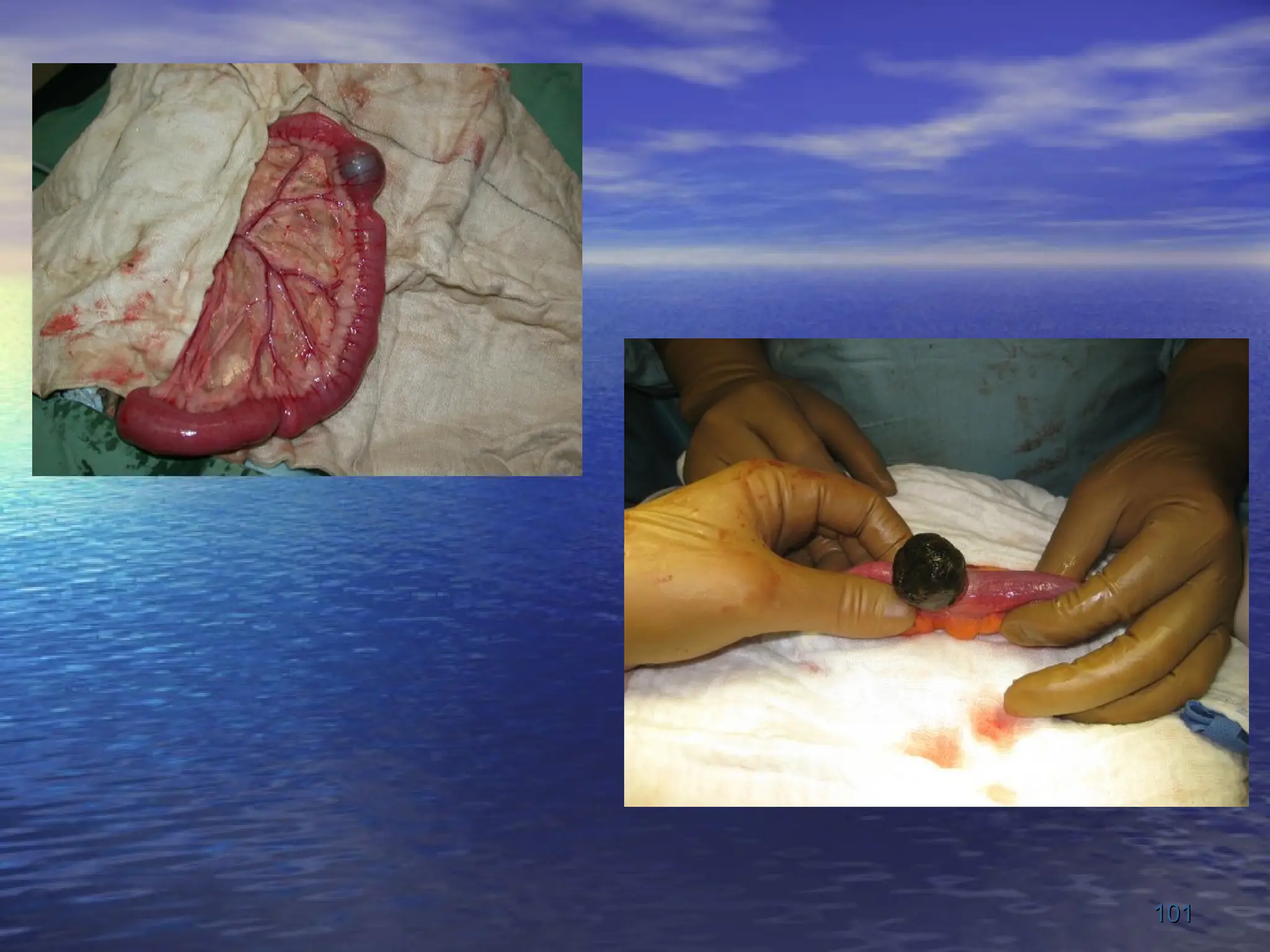
I. Gallstones: Gallstone Ileus (stones enter the
intestine through a fistulous communication
between the bile duct and the GI tract)
II. Food: Bolus obstruction may occur after partial or
total gastrectomy when unchewed articles can
pass directly into small bowel
III. Bezoars: Trichobezoars (Hair Balls) and
Phytobezoar (Fruit/Vegetable Fibre).
IV. Worms: Ascaris lumbricoides may cause low small
bowel obstruction particularly in children, the
institutionalized and those near the tropics.
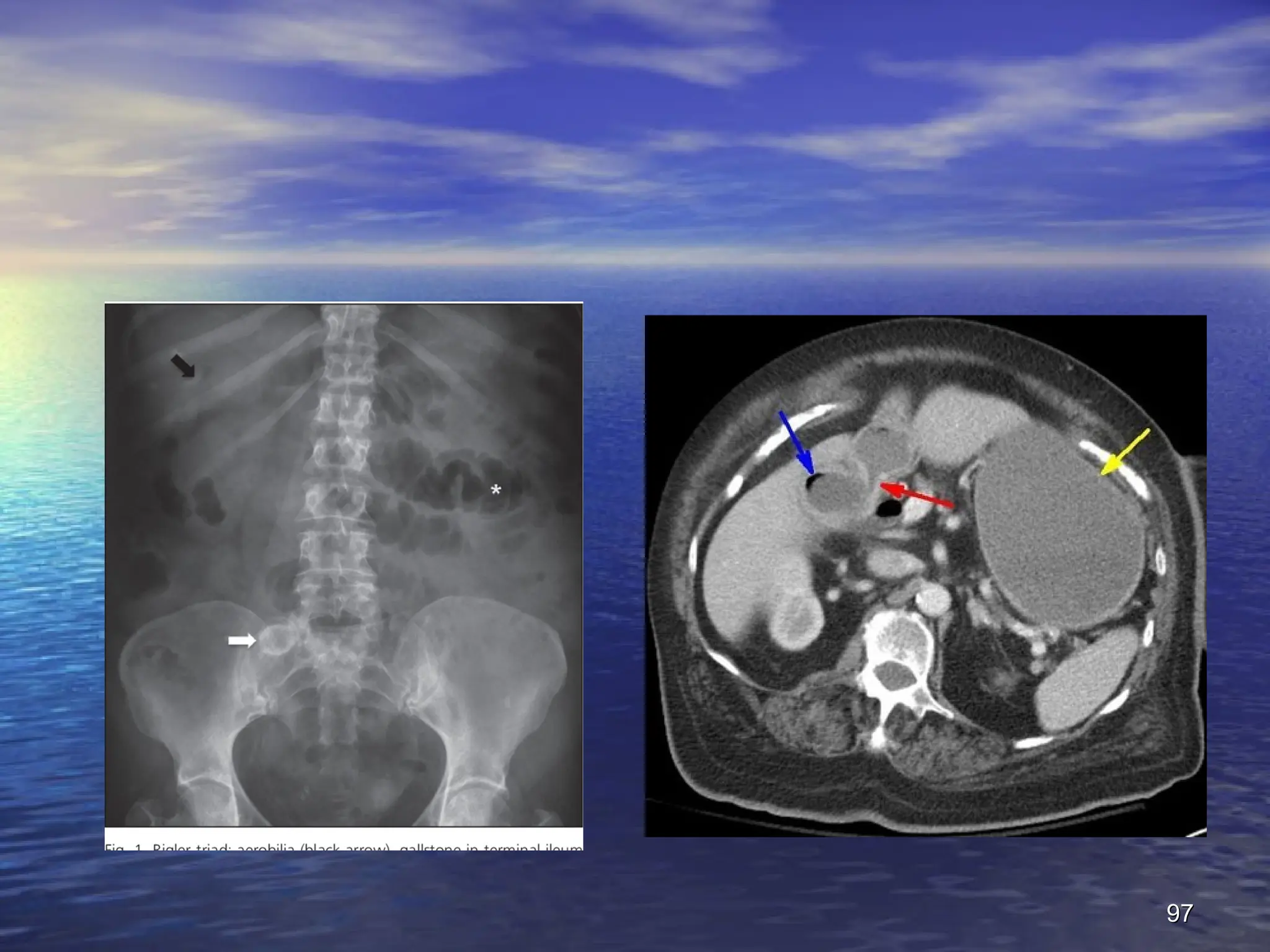
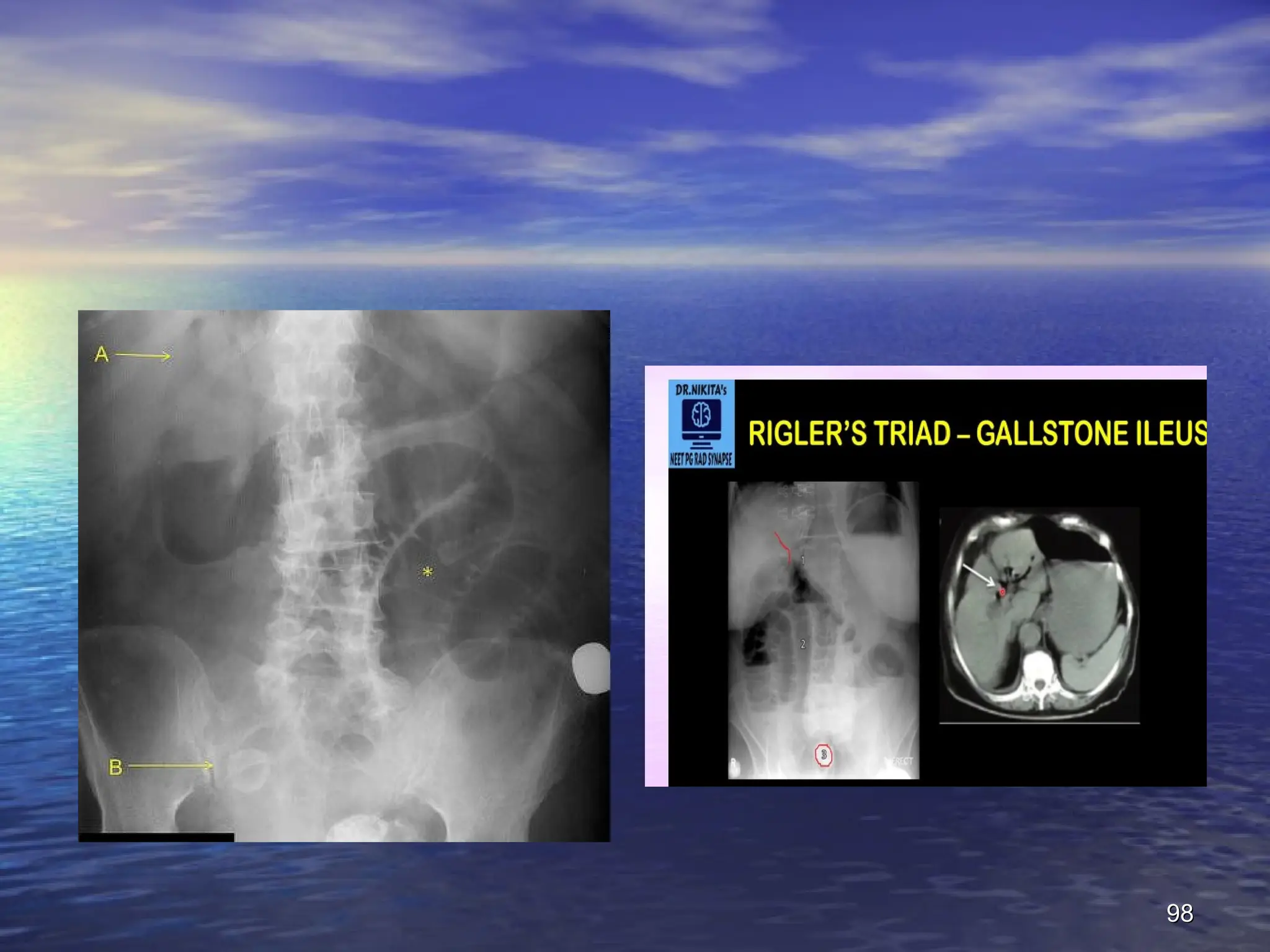
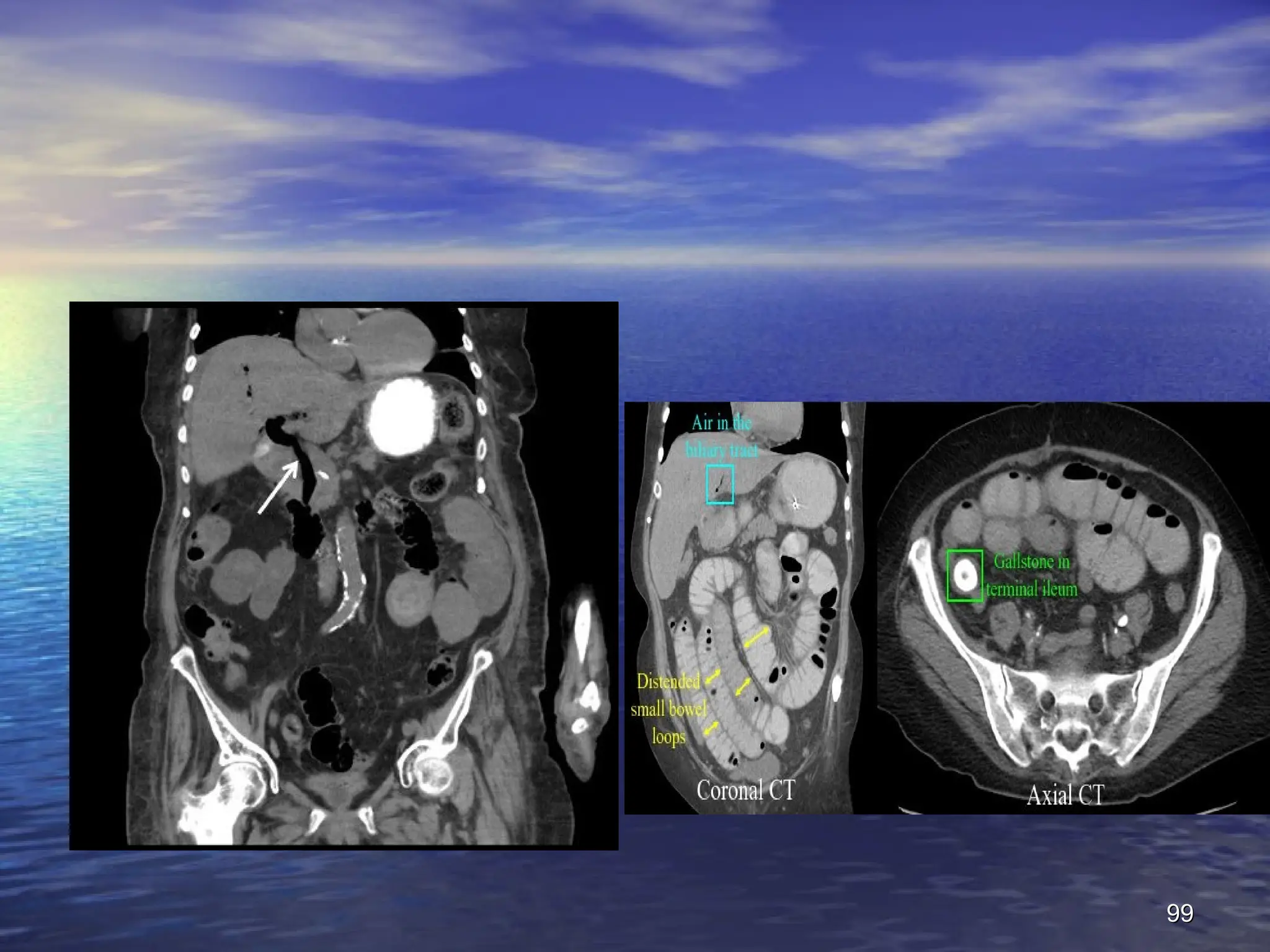
96.
Radiography
Radiography
- :
- :
Thecharacteristic radiological sign of gallstone ileus
The characteristic radiological sign of gallstone ileus
is
is
Rigler's triad
Rigler's triad
:
:
small bowel obstruction
small bowel obstruction +
+ pneumobilia
pneumobilia +
+ atypical
atypical
mineral shadow on radiograp ectopic calcified
mineral shadow on radiograp ectopic calcified
gallstone, usually in the right iliac fossa
gallstone, usually in the right iliac fossa
Presence of two of these radiological signs has been
Presence of two of these radiological signs has been
considered pathognomic of gallstone ileus
considered pathognomic of gallstone ileus
.
.
96
96
Treatment
Treatment
:
:
Laparatomy & thestone is milked proximally away
Laparatomy & the stone is milked proximally away
from the site of impaction, the intestine is
from the site of impaction, the intestine is
opened at this point and the gallstone removed
opened at this point and the gallstone removed
.
.
If the gallstone is faceted, a careful check for other
If the gallstone is faceted, a careful check for other
enteric stones should be made
enteric stones should be made
.
.
The region of the gall bladder should not be
The region of the gall bladder should not be
explored
explored
.
.
100
100
2
2
-
-
Food
Food
:
:
Occur after partialor total gastrectomy when
Occur after partial or total gastrectomy when
unchewed articles can pass directly into small
unchewed articles can pass directly into small
bowel
bowel
.
.
The management is similar to that for gallstone,
The management is similar to that for gallstone,
with intraluminal crushing usually successful
with intraluminal crushing usually successful
.
.
102
102
103.
3
3
-
-
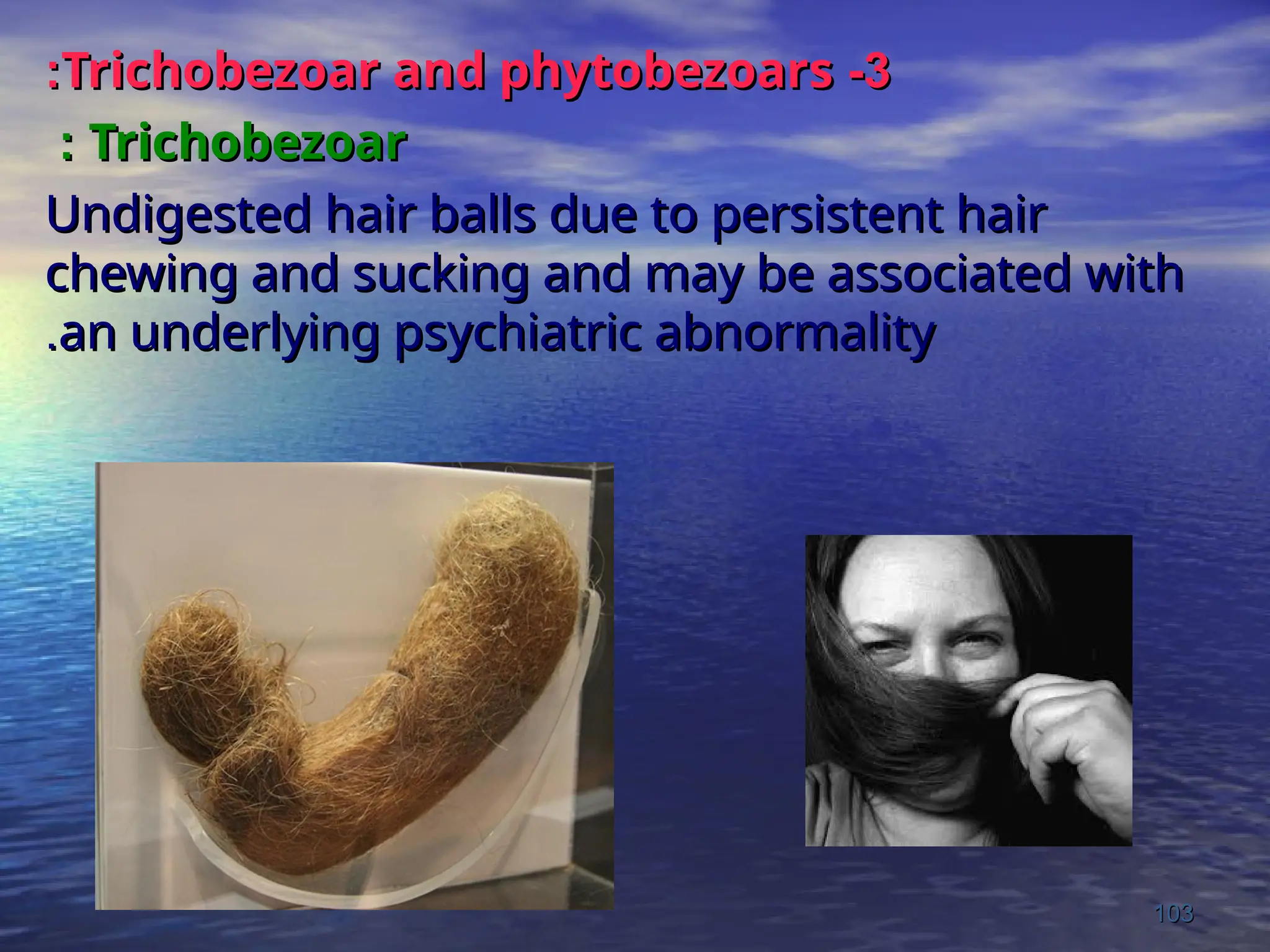
Trichobezoar and phytobezoars
Trichobezoarand phytobezoars
:
:
Trichobezoar
Trichobezoar
:
:
Undigested hair balls due to persistent hair
Undigested hair balls due to persistent hair
chewing and sucking and may be associated with
chewing and sucking and may be associated with
an underlying psychiatric abnormality
an underlying psychiatric abnormality
.
.
103
103
104.
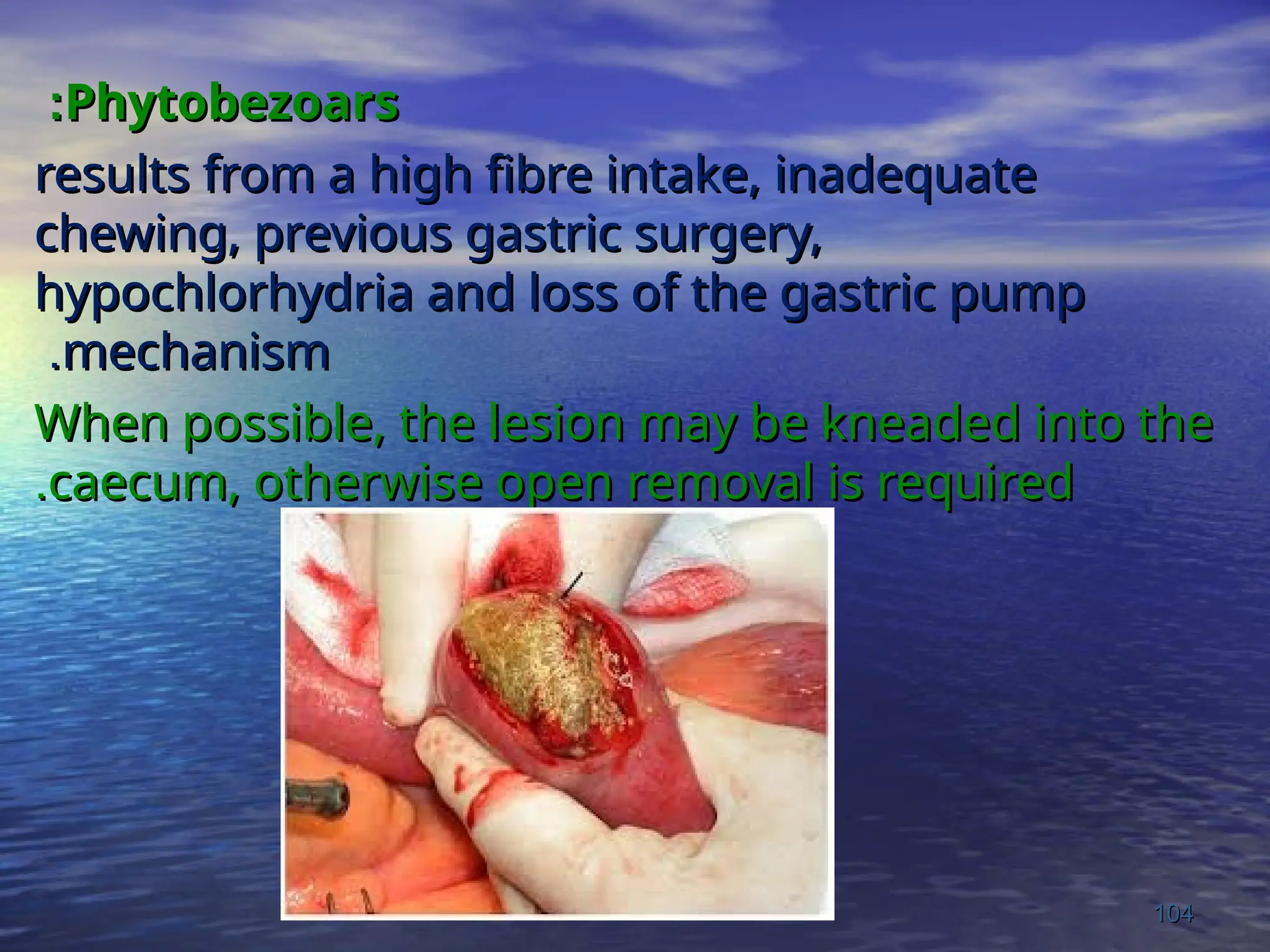
Phytobezoars
Phytobezoars
:
:
results from ahigh fibre intake, inadequate
results from a high fibre intake, inadequate
chewing, previous gastric surgery,
chewing, previous gastric surgery,
hypochlorhydria and loss of the gastric pump
hypochlorhydria and loss of the gastric pump
mechanism
mechanism
.
.
When possible, the lesion may be kneaded into the
When possible, the lesion may be kneaded into the
caecum, otherwise open removal is required
caecum, otherwise open removal is required
.
.
104
104
105.
5
5
-
-
Worms
Worms
:
:
Ascaris lumbricoides maycause low SBO
Ascaris lumbricoides may cause low SBO
particularly in chidren, an attack frequently
particularly in chidren, an attack frequently
follow initiation of anti-helminthic therapy
follow initiation of anti-helminthic therapy
.
.
At laparatomy it may be possible to knead the
At laparatomy it may be possible to knead the
tangled mass into the caecum, If not it should be
tangled mass into the caecum, If not it should be
removed
removed
.
.
105
105
106.
SBO due to
SBOdue to Ascaris lumbricoides
Ascaris lumbricoides
.
.
106
106
107.
Internal Hernia
Occurswhere a portion of the small
intestine becomes entrapped in one of the
retroperitoneal fossae or into a congenital
mesenteric defect.
In the absence of adhesions hernia is
uncommon to cause obstruction and a
preoperative diagnosis is unusual.
The standard treatment for a hernia is to
release the constricting agent by division.
108.
Obstruction from EntericStrictures
Small bowel strictures usually occur secondary
to Tuberculosis or Crohn’s disease.
Malignant strictures associated with lymphoma
are common, whilst carcinoma and sarcoma
are rare.
Presentation is usually Subacute or Chronic.
Standard surgical management consists of
resection and anastomosis.
109.
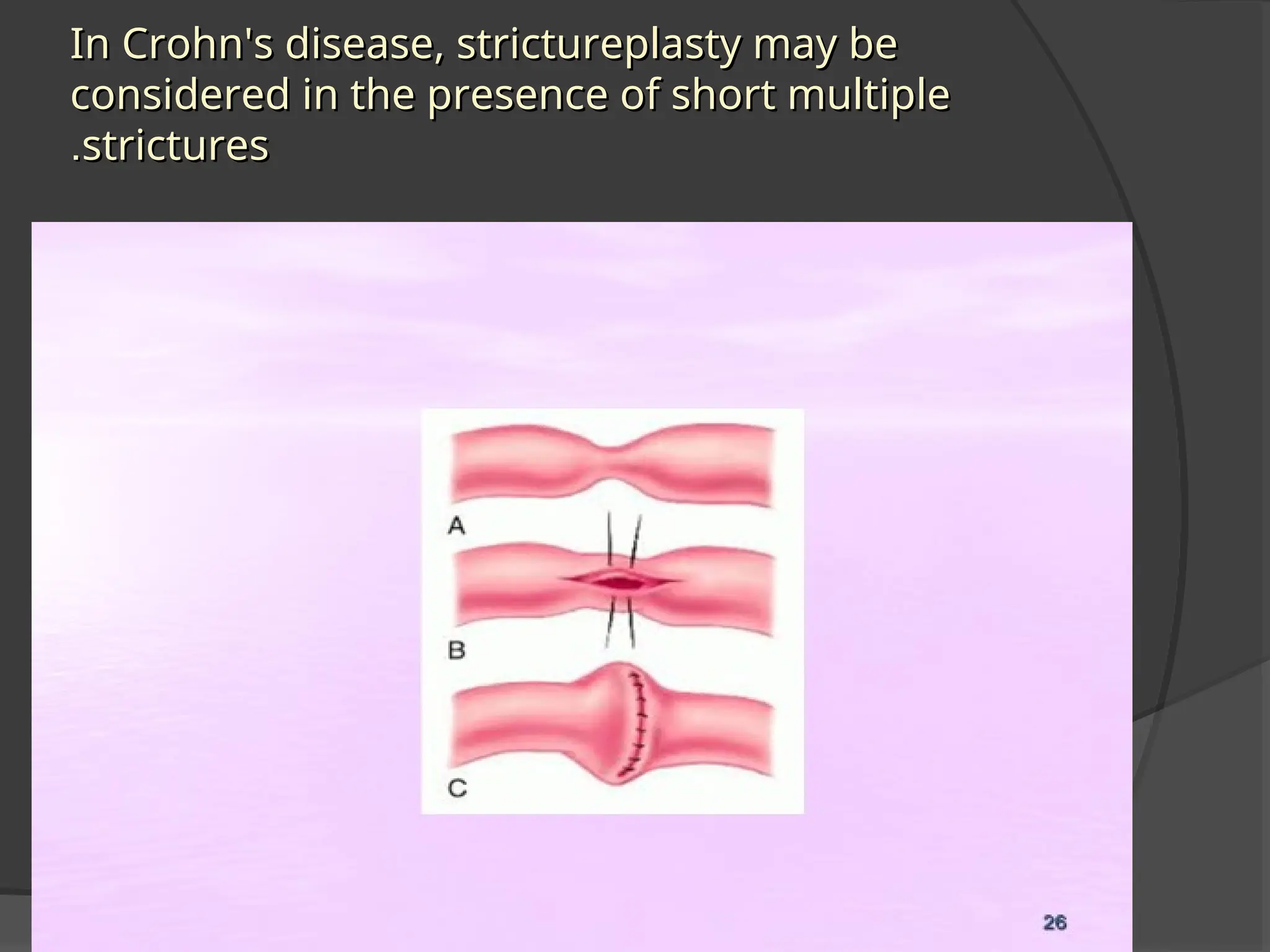
In Crohn's disease,strictureplasty may be
In Crohn's disease, strictureplasty may be
considered in the presence of short multiple
considered in the presence of short multiple
strictures
strictures
.
.
110.
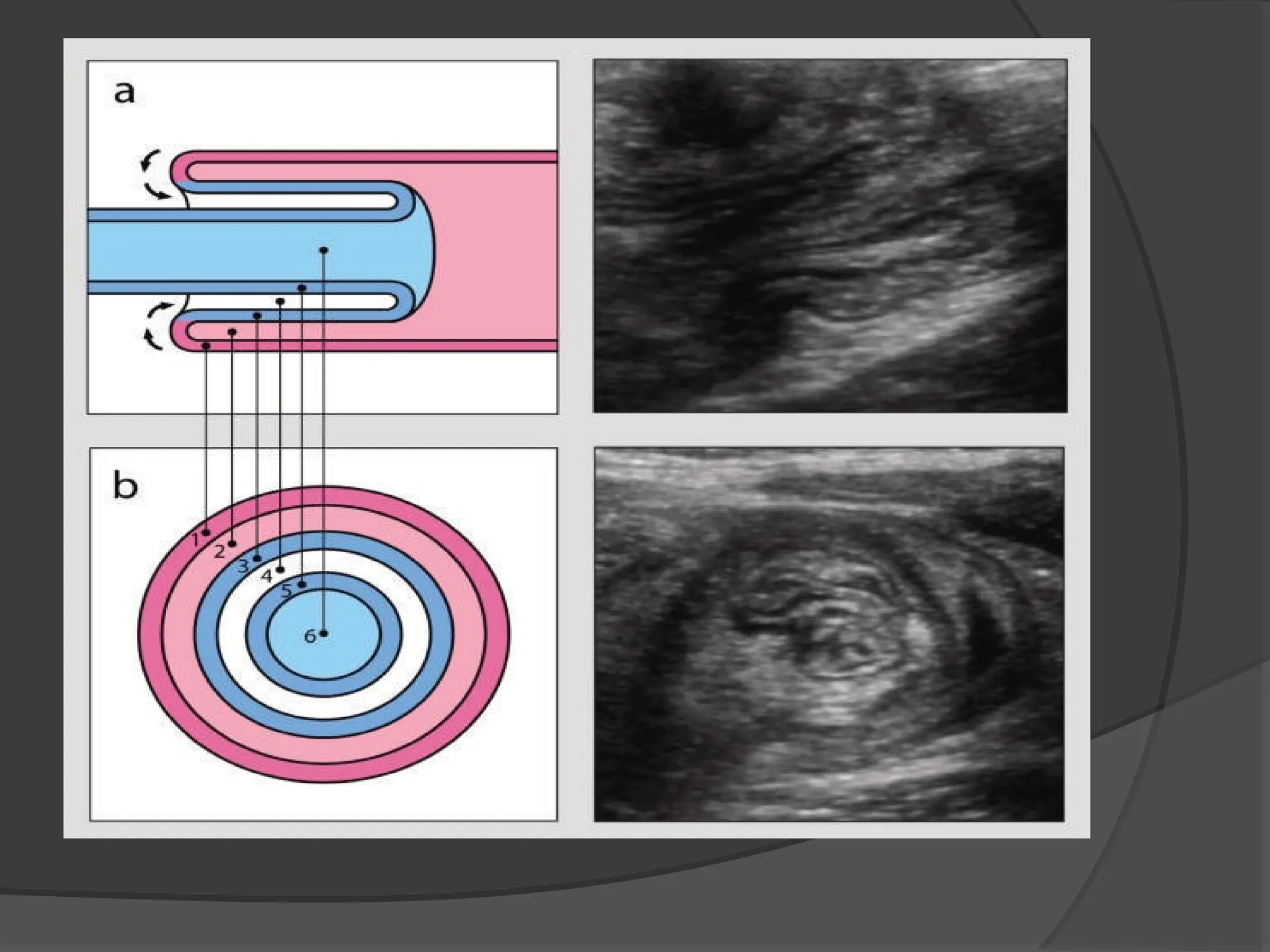
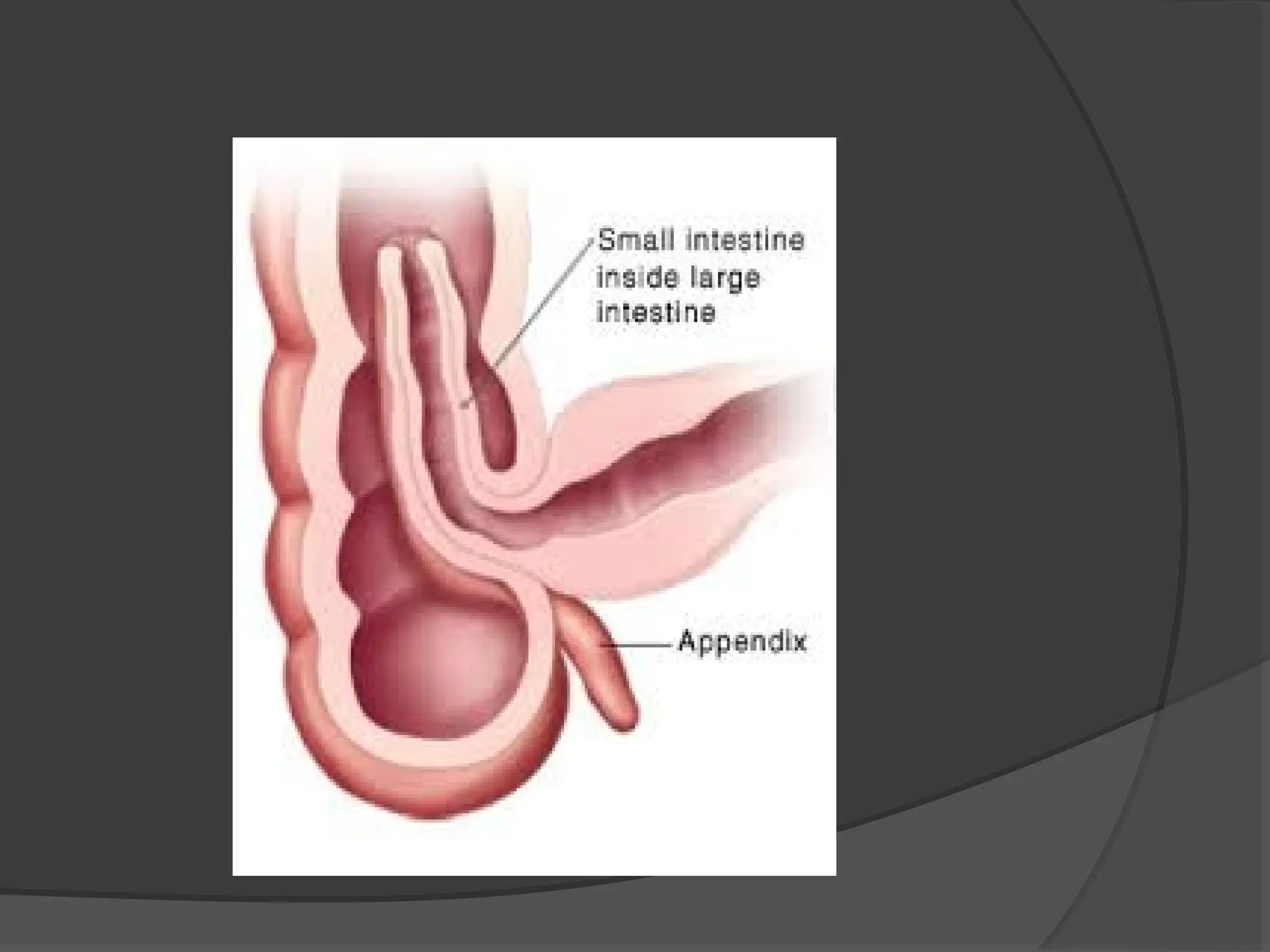
Acute Intussusception
Mostcommon in children.
Primary or secondary to intestinal
pathology, e.g. polyp, Meckel's
diverticullum.
Ileocolic is the most common variant.
Can lead to an ischemic segment and
strangulation.
Paralytic ileus
Definition:A state in which there is failure of
transmission of peristaltic wave secondary to
neuromuscular failure
This will leads to signs of intestinal obstruction due to
accumulation of gas and fluid in the bowel with signs of
abdominal distension ,constipation, but NO Pain.
Varieties :
1. Post operative: - Self limiting, Lasts for 24-72 Hours
2. Infection: Peritonitis
3. Reflex ileus: as in fracture of the spine or ribs on in
retroperitoneal hemorrhage
4. Metabolic : Hypokalemia, DM
5. Drugs : Spasmolytic Drugs , Parkinson Drugs, Atropine
121.
Clinical features:
-Ittakes clinical significance if there has
been no return of normal bowel sound
and no passage of flatus after 72 hrs of
Surgery
- Abdominal distension is marked,
Effortless Vomiting, but pain is NOT a
feature
-Radiologically: Multiple Fluid Level
122.
Management :
1.General principles must be applied if the disease
takes place
2. Remove the cause
3. Relieve GI distension by decompression
4. Monitoring fluid and electrolyte balance
5. Rarely medical agents are used (AntiCholene
Esterase)
6. Laparotomy after 72 hours
123.
Pseudo-Obstruction
This conditiondescribes an obstruction,
usually of the colon, in the absence of a
mechanical cause or acute intra-
abdominal disease.
It is associated with a variety of
syndromes where there is an underlying
neuropathy and/or myopathy.
124.
1) Small intestinalpseudo-obstruction
• This condition may be primary or
secondary.
• The clinical picture consists of recurrent
subacute obstruction.
• The diagnosis is made by the exclusion
of a mechanical cause.
• Treatment consists of initial correction
of any underlying disorder.
125.
2) Colonic pseudo-obstruction.
•This may occur in an acute or a chronic
form.
• The acute form is known as Ogilvie
syndrome, presents as acute large bowel
obstruction.
• Abdominal radiographs show evidence of
colonic obstruction with marked caecal
distension being a common feature
• Perforation is a common complication.
• Treated by colonoscopic decompression

![Incidence
Site of Obstruction Cause Relative Incidences
(%)
Small intestine [85%] Adhesions 60
Hernia 15
Tumors 15
miscellaneous 10
Large Intestine [15%] CA colon 65
Diverticulitis 20
Volvulus 5
miscellaneous 10](https://image.slidesharecdn.com/19-intestinalobstruction01-08-15-0822-08-243-251018130819-5d6541d0/75/19-Intestinal-Obstruction-01-08-15-08-22-08-24-3-ppt-13-2048.jpg)