1. The document discusses gastrointestinal bleeding, describing its various presentations including hematemesis, melena, hematochezia, occult blood in stools, and chronic blood loss/anemia.
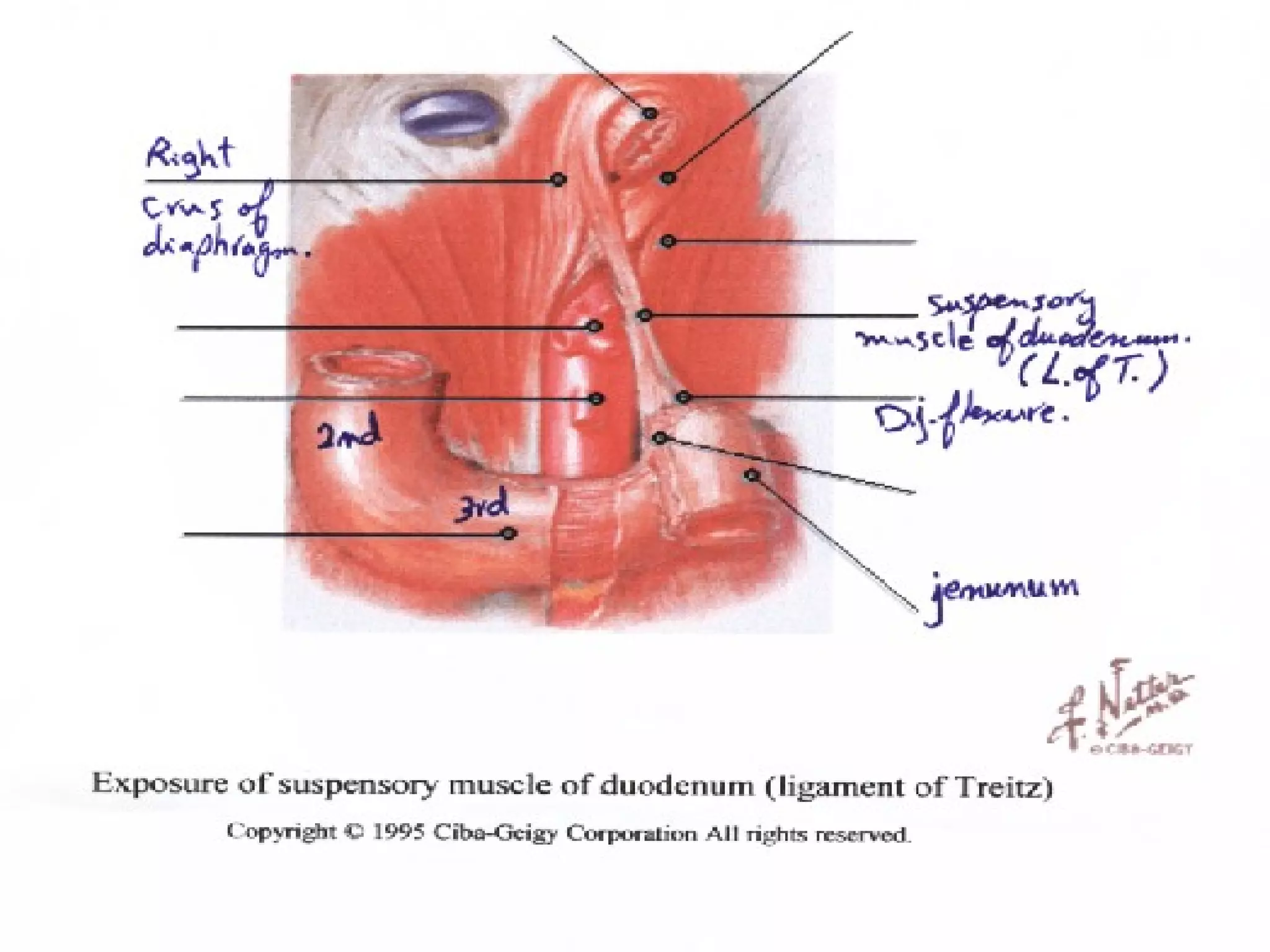
2. Upper GI bleeding occurs above the ligament of Treitz and can cause hematemesis or melena, while lower GI bleeding occurs below and causes melena and hematochezia but no hematemesis.
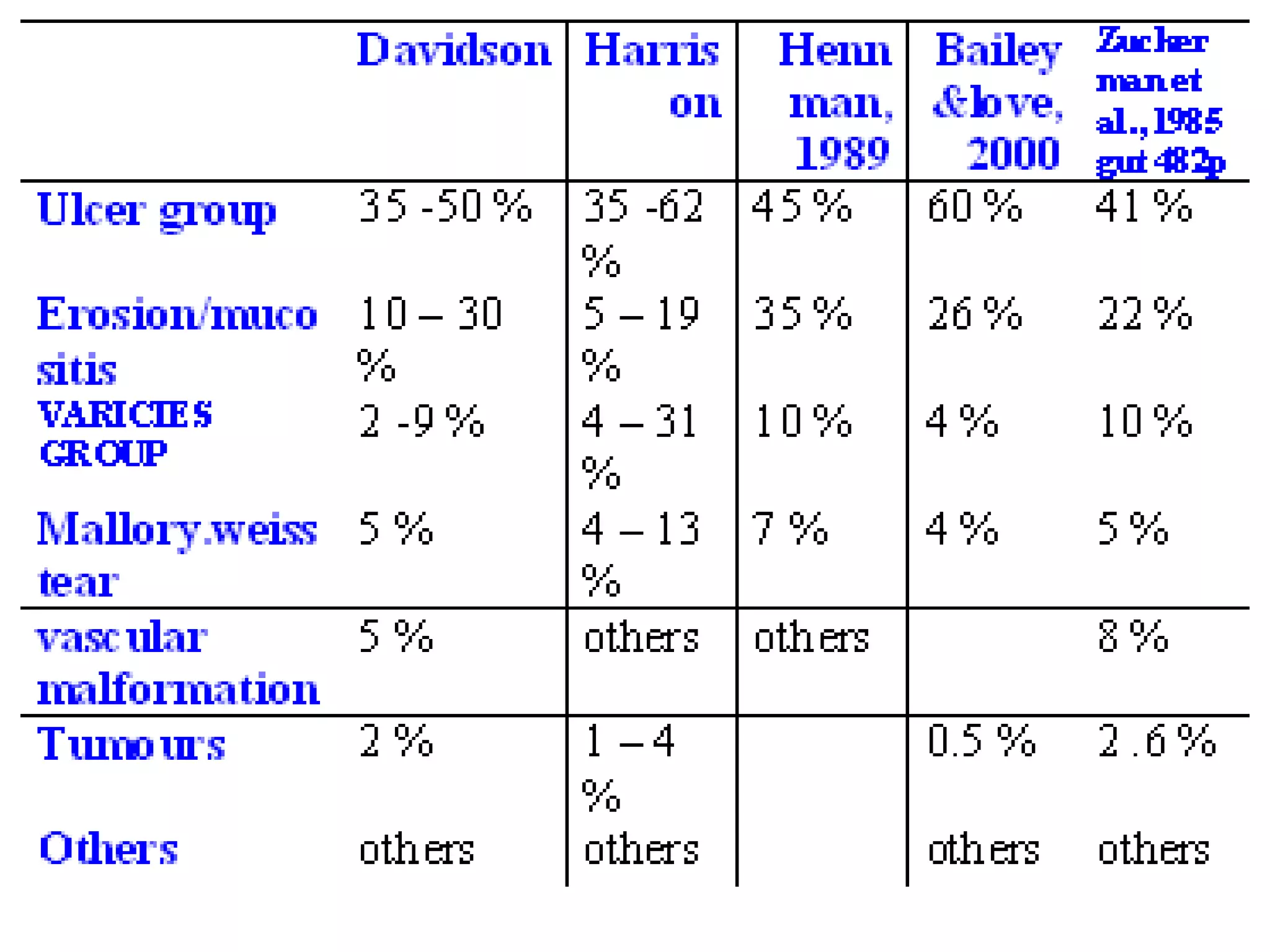
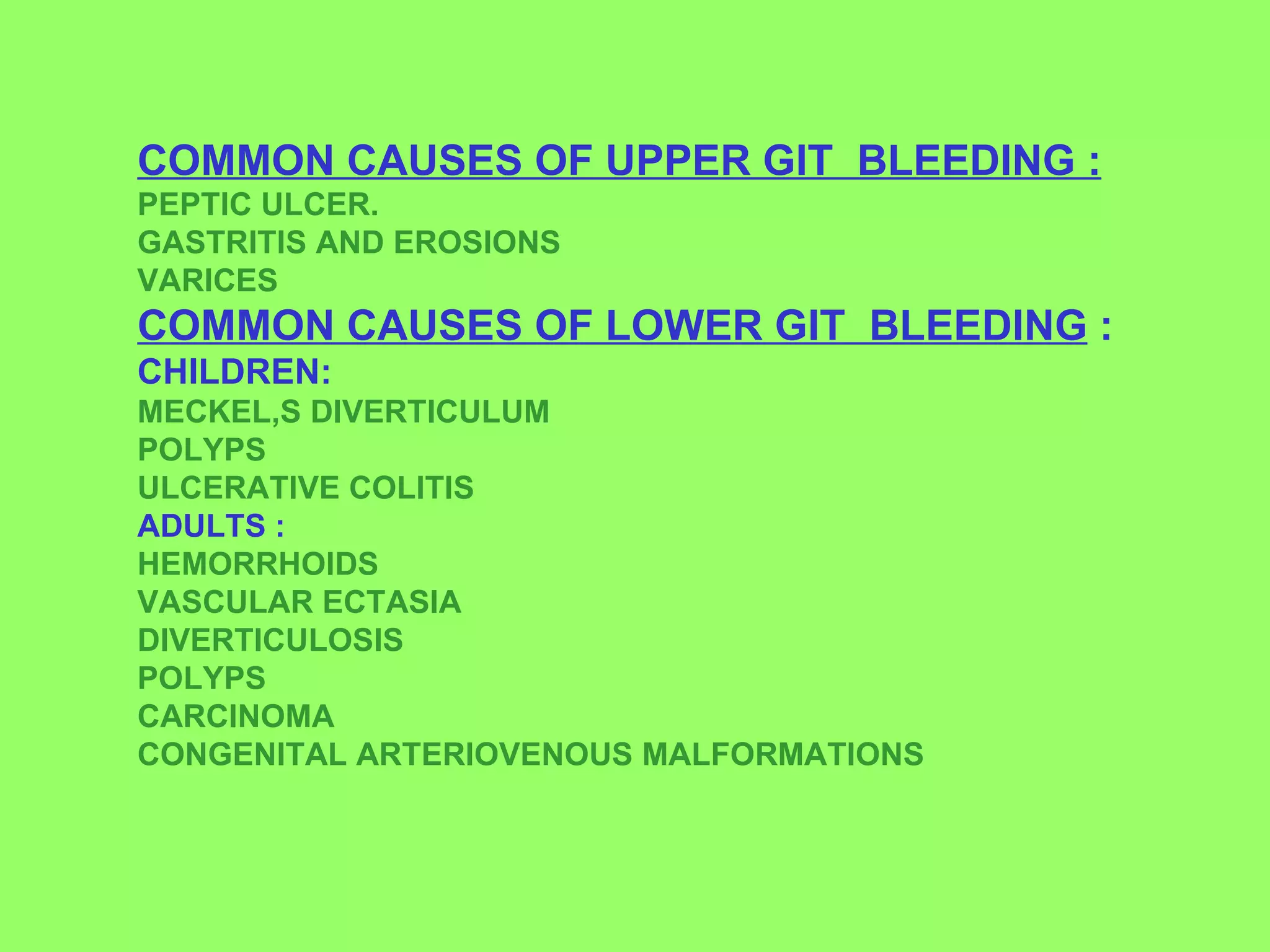
3. Common causes of upper GI bleeding include peptic ulcer disease, gastritis, and esophageal varices, while common causes of lower GI bleeding include hemorrhoids, diverticulosis, and polyps.
![بسم اللله الرحمن الرحيم Gastrointestinal bleeding Draz MY , Egypt 2008 Mb. Bch, D. Sc (Alazhar) .,M. Sc (Cairo) ,M. Sc (Ain shams). Surgeon ,Internist, Emergency Registrar. [email_address]](https://image.slidesharecdn.com/cusersmohameddesktopacuteacutegastrointestinalbleedingdrazmyegypt2009-090929184948-phpapp01/75/acute-gastrointestinal-bleeding-hematemesis-melena-1-2048.jpg)