Downloaded 133 times

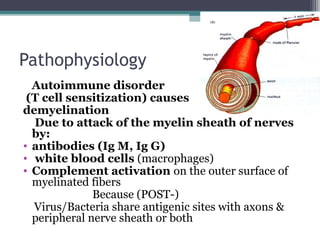
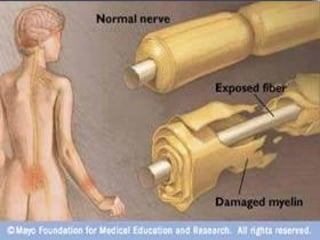
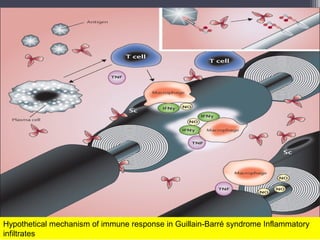
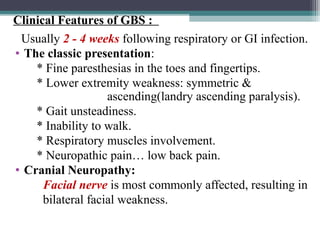
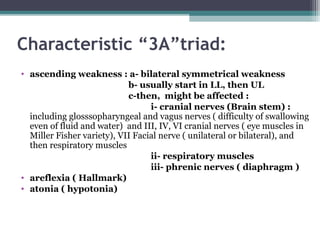

The document describes a case of acute flaccid paralysis (AFP) in a 12-year-old male who presented with pain and weakness in his lower limbs. On examination, he had hypotonia, hyporeflexia, and reduced motor strength in both upper and lower limbs. Guillain-Barré syndrome (GBS) is the most common cause of AFP and involves demyelination of peripheral nerves due to autoimmune attack. Key diagnostic features of GBS are rapid onset of symmetric ascending paralysis, intact sensation, absence of fever or cranial nerve involvement, and albuminocytologic dissociation on CSF analysis. Treatment involves hospitalization, IV immunoglobulin or plasmapher























































































