Downloaded 205 times



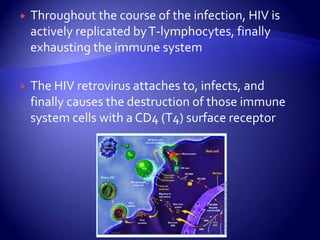

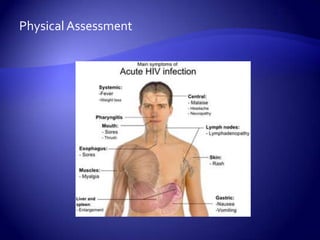
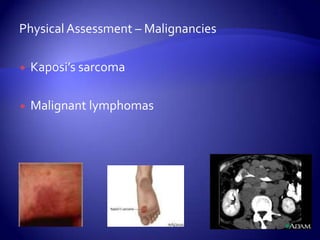


The document provides an overview of interventions for clients with HIV/AIDS. It begins with key terms related to immunodeficiency and HIV/AIDS. It then describes the pathophysiology and etiology of HIV, how it is transmitted, and methods for preventing transmission. Nursing assessments, diagnoses, outcomes, and interventions are outlined with a focus on managing infections, nutritional status, and psychosocial needs. The document concludes with references.






























































































