Downloaded 383 times

![pH Review
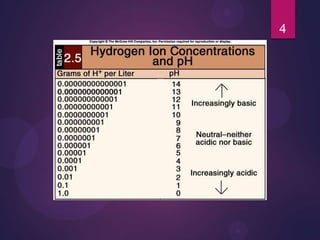
pH = - log [H+]
H+ is really a proton
Range is from 0 - 14
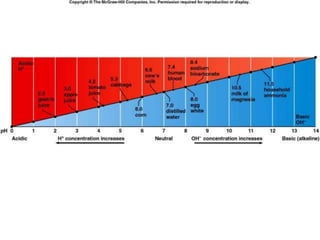
If [H+] is high, the solution is acidic; pH < 7
If [H+] is low, the solution is basic or alkaline ; pH >
7
2](https://image.slidesharecdn.com/acidandbase-130906083717-/85/acid-base-balance-and-imbalance-2-320.jpg)
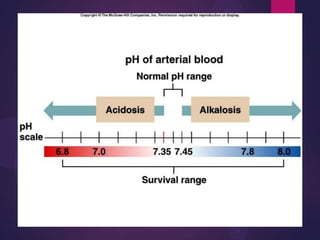
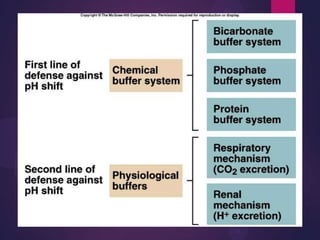
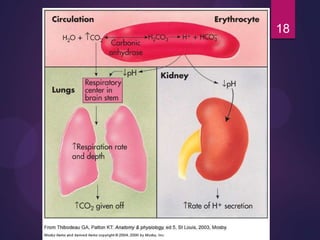




The document provides an overview of acid-base balance in the human body, detailing the definitions of acids and bases, their effects on pH levels, and the significance of homeostasis. It explains the mechanisms the body uses to maintain pH, including buffer systems, respiratory regulation, and renal excretion, while also discussing the consequences of acidosis and alkalosis. The document further outlines the symptoms, treatments, and diagnostic approaches for various acid-base imbalances.























































































