Downloaded 11 times




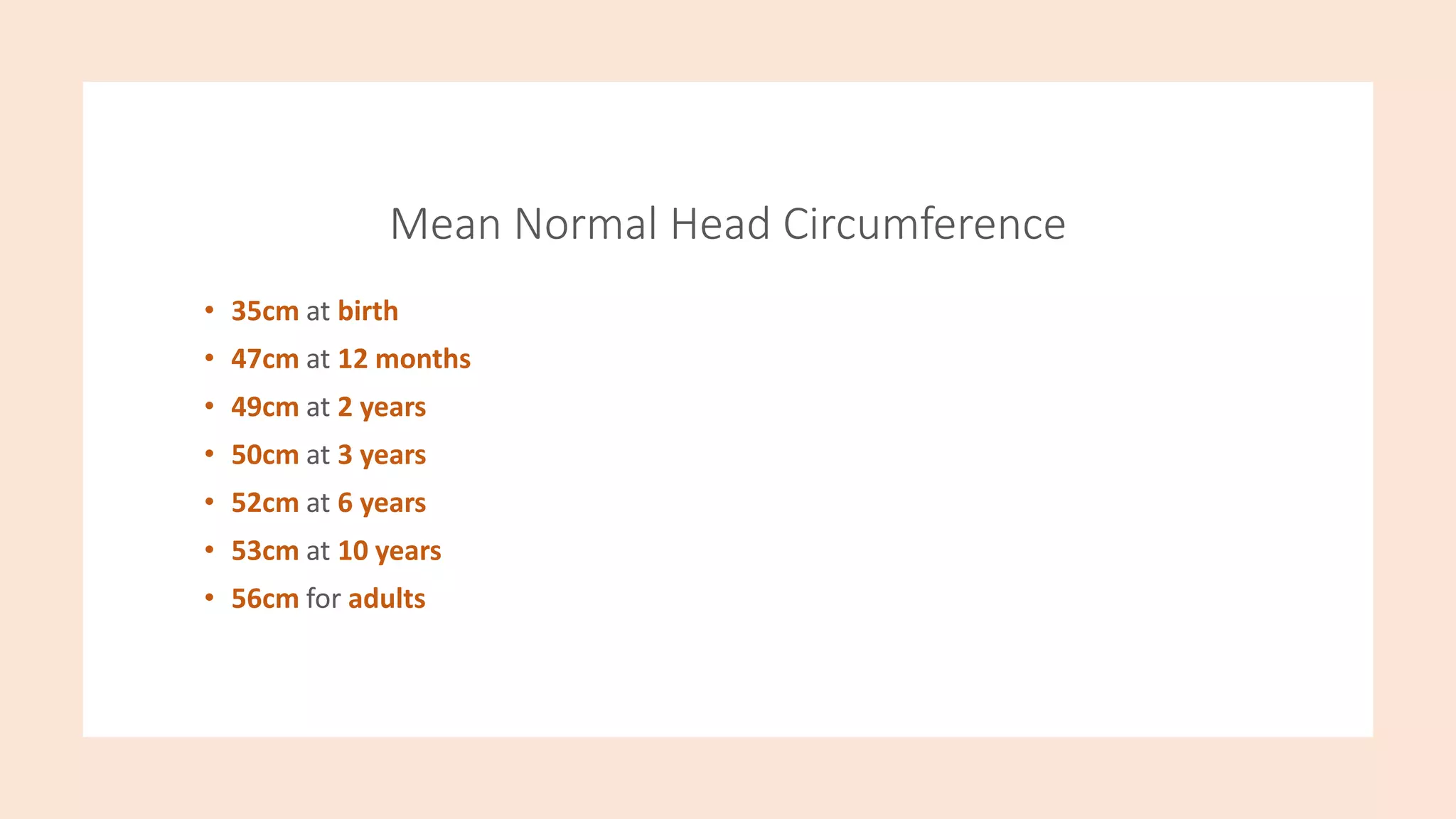




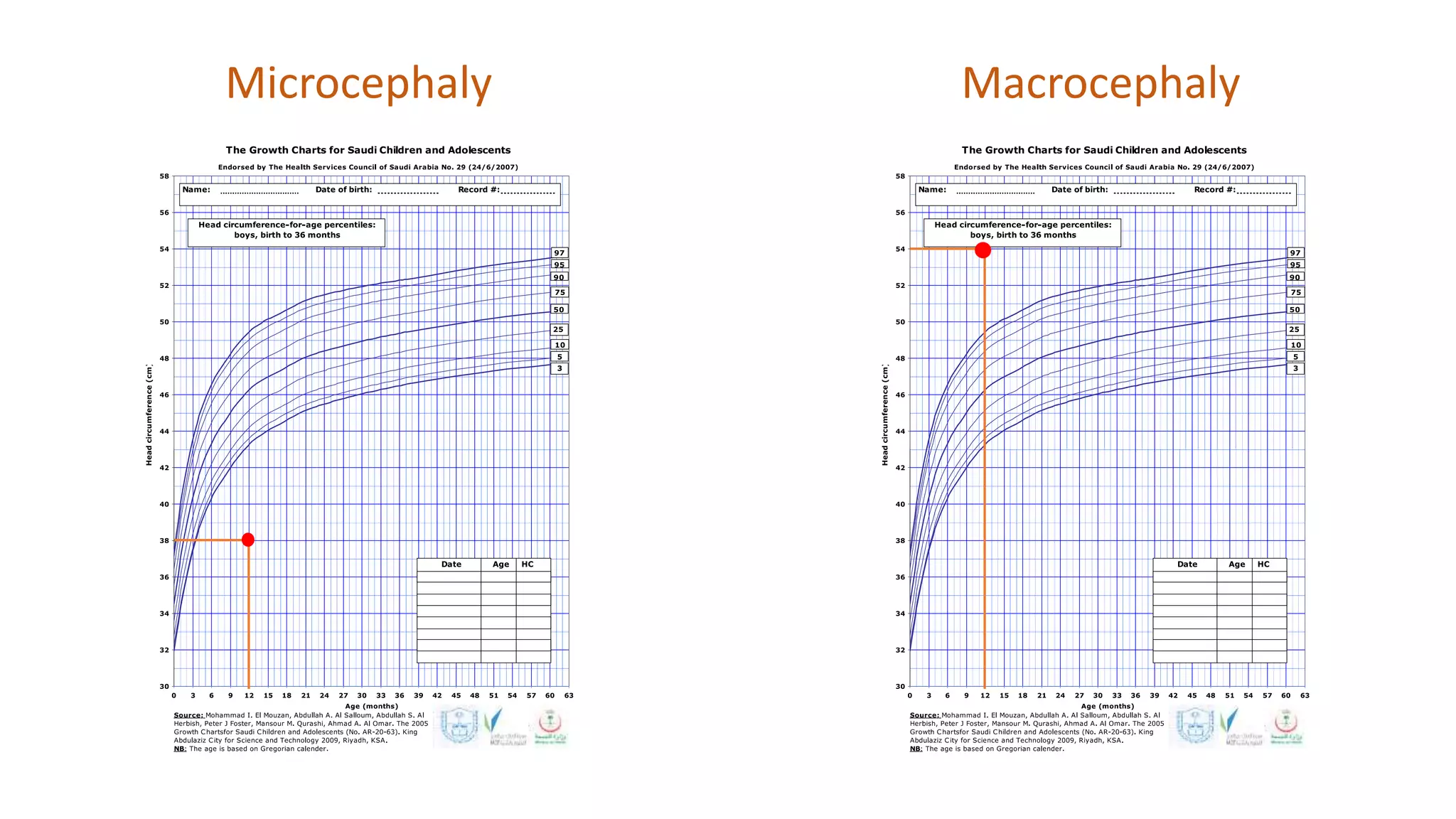






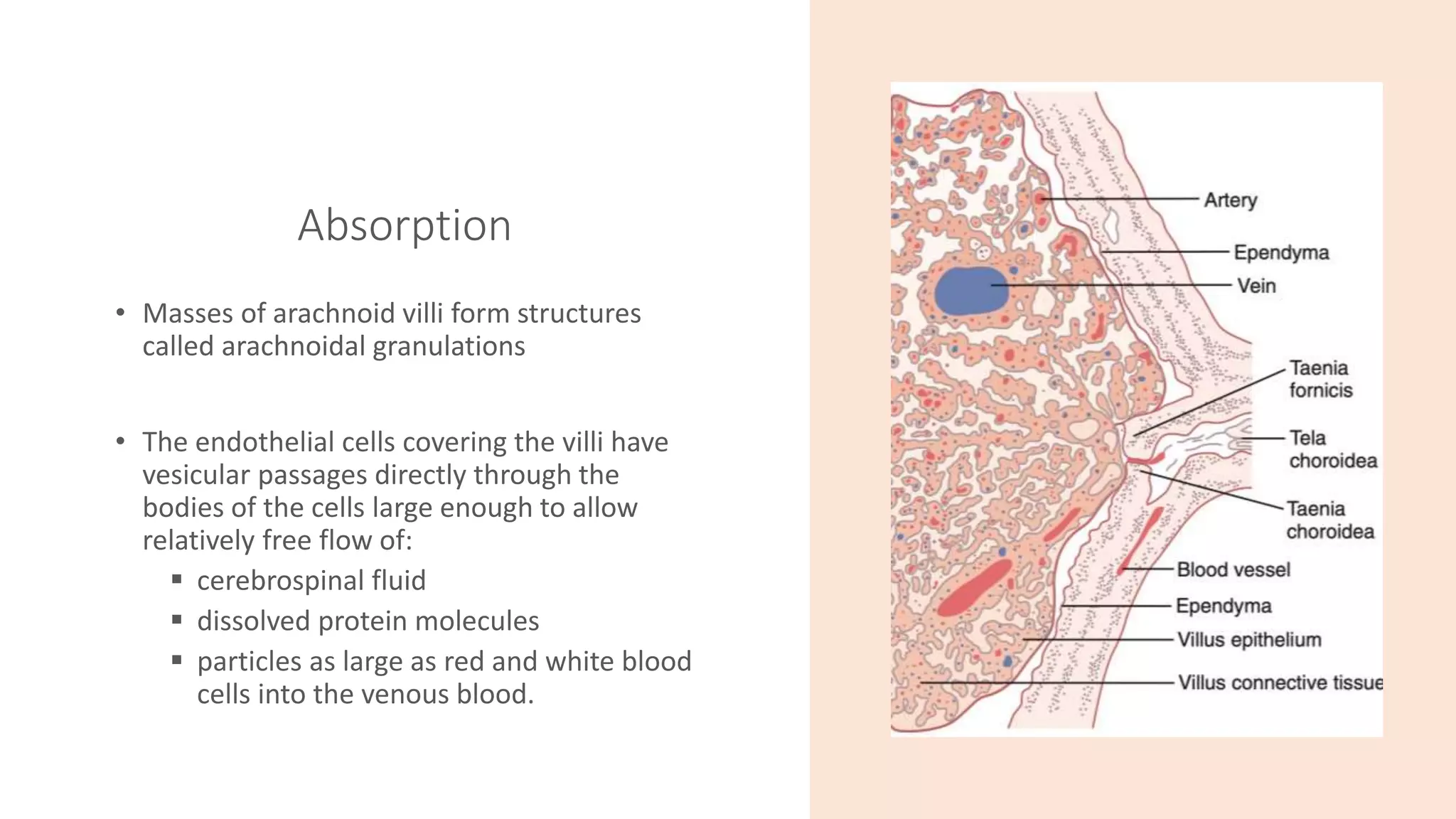

















The document discusses normal head growth and measurement, cerebrospinal fluid physiology and circulation, and the clinical approach to infants with abnormal head sizes. Key points include: head circumference should be measured regularly from birth to age 2-3 years and plotted on a growth chart; cerebrospinal fluid is produced in the brain ventricles and absorbed through arachnoid granulations; microcephaly is defined as a head circumference below the 2nd percentile and can be caused by genetic or acquired factors, while macrocephaly is above the 98th percentile and can be due to increased brain, blood, or fluid volume or intracranial pressure. A full history and physical exam is needed to evaluate the cause in infants with