Download to read offline

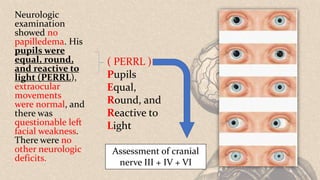
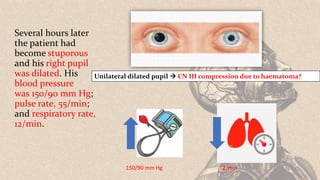
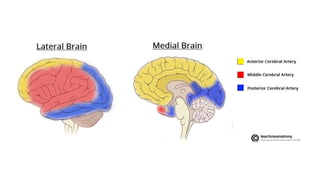
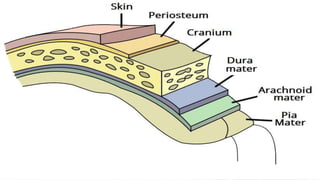
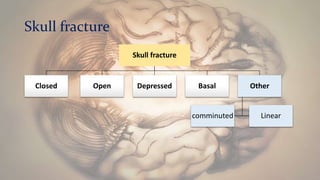
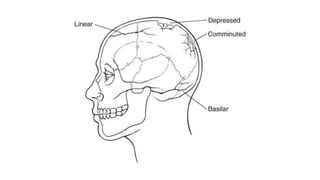

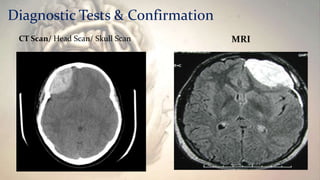
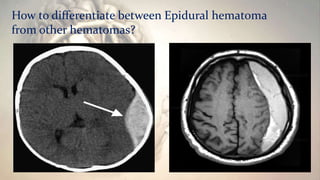
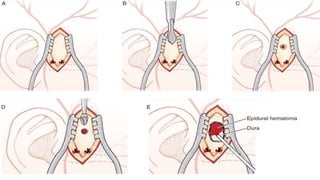


A 21-year-old motorcyclist was brought to the emergency room after being found unconscious on the street with a head injury. He had swelling above his right ear. Initially his neurological exam was normal except for some confusion and unclear speech. Later he became stuporous and his right pupil dilated. Emergency surgery was undertaken. The document discusses the anatomy of the brain, cranial meninges, types of head injuries including epidural hematoma. It describes the signs and symptoms of epidural hematoma, methods of diagnosis including CT scan, and treatment involving craniotomy or burr hole evacuation surgery.












![Stroke [uncensored] - by MHR Corporation](https://cdn.slidesharecdn.com/ss_thumbnails/mhr4-stroke-101129110104-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
































































