
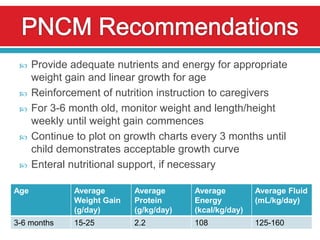
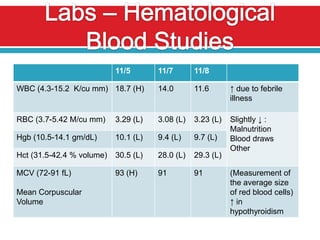
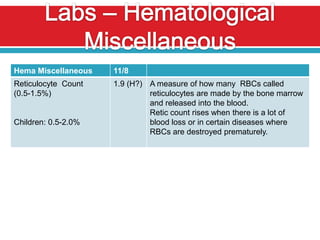
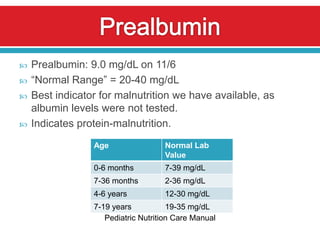
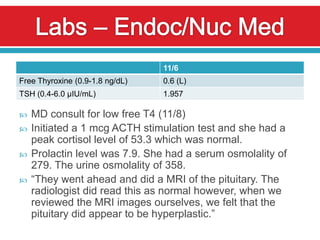
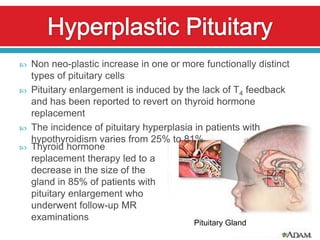

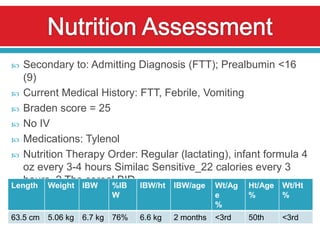
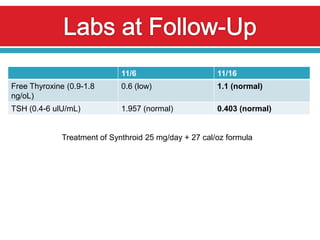
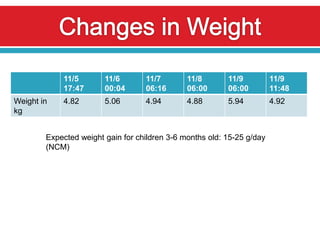

A 5-month-old female infant presented with fever and vomiting and was diagnosed with failure to thrive and an acute febrile illness. Labs showed hypothyroidism and malnutrition. The patient was started on levothyroxine and a higher calorie formula. After one week of treatment, the patient's thyroid levels normalized and intake improved, though the family was counseled to further increase calorie intake to support adequate growth.



































































