Definition
• It denotesan occipitofrontal circumference (OFC) 3
or more standard deviations below the mean for the
individual’s age and gender.
• Craniosynostosis - results from premature fusion of
1 or more sutures results in a small head size with
abnormal head shape which should be
distinguished from microcephaly.
3.
Types
• Primary (genetic)
–Familial
• AD –mild forehead slant, prominent ears and borderline MR
• AR –typical appearance with slanted forehead ,prominent
nose and ears, severe MR
– Genetic syndromes-Down, other trisomies, cri-du chat,
Cornelia de Lange, Rubinstein-Taybi
4.
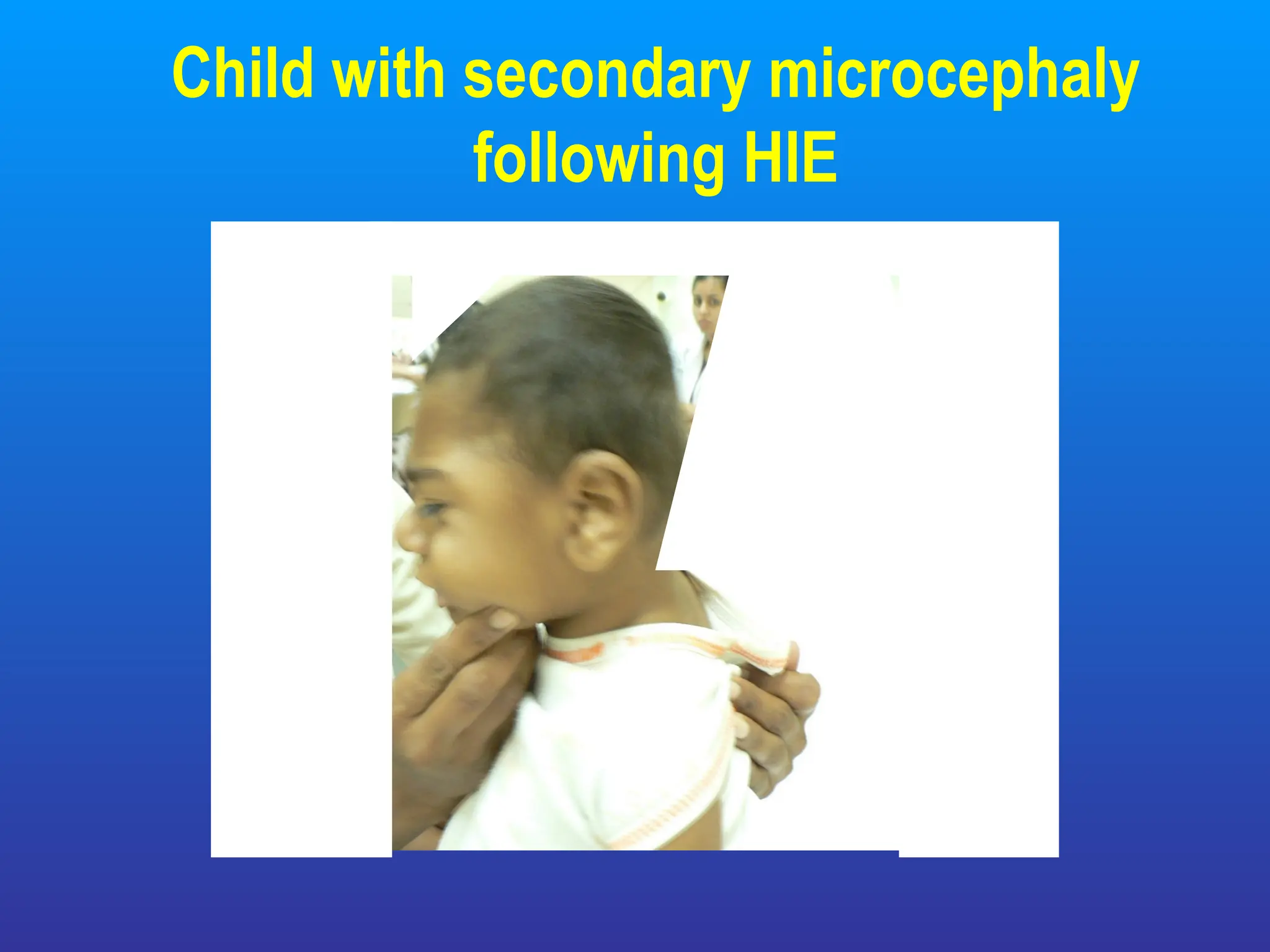
Types – Contd..
•Secondary (non-genetic)-if noxious agent affects brain
growth in utero upto 1st
2 years of life.
– Hypoxic-ischaemic encephalopathy
– Intrauterine infections
– CNS infections
– Fetal hydantoin syndrome (mother takes phenytoin in pregnancy)
– Malnutrition
– Metabolic( maternal PKU)
Evaluation - History
•Antenatal history-maternal hyperthermia, exposure
to radiation, exanthematous febrile illness
• Family history of small head/MR/seizures.
• Post natal CNS infections particularly in 1st
2 years
of life.
• OFC at birth
8.
Measuring OFC
• Afibroelastic / metal measuring tape is placed
around the head at the full points
– Occipital protuberance posteriorly
– Nasion anteriorly
– Measurement is made by overlap over the temporal
bone.
9.
Examination
• OFC-plotted ina chart and compared for the norms
(age and sex).
• Serial OFC records desirable-rate of growth
• Abnormal head shape, fontanelle & sutures
• Stigmata of intrauterine infections
• Dysmorphism
• Detailed neurological examination
10.
Investigations
• Neuroimaging -CT/MRI of the brain help identify
structural defects.
• TORCH titers for intrauterine infections
• Karyotype if chromosomal syndrome/ associated
congenital malformation
• Maternal phenylalanine levels (for PKU)
• Fetal USG-for fetal head size particularly if family
history present
11.
Treatment
• Per sehead size cannot be changed by treatment
• Associated delay needs to be addressed
– Stimulation programme
– Special schools
• Treatment of hearing/vision impairment if present
• Treatment of seizures if present
#2 There are separate norms of head growth for girls and boys. Two standard deviations is taken as it represents a value statistically beyond the normal range. Some consider less than 3 SD as microcephaly.
#3 Primary –have no other malformations .usually follow a mendelian pattern of inheritance or are chromosomal. Head circumference is small at birth.
MR-mental retardation
#4 Primary – have no other malformations .usually follow a mendelian pattern of inheritance or are chromosomal. Head circumference is small at birth.
#9 Small OFC at birth usually indicates a process that has started early in intrauterine life. It is usually seen in primary microcephaly.
Determination of cause helps in giving a prognosis and in genetic counselling
#10 Laboratory investigations would be directed by the history and examination. Usually neuroimaging is indicated.