Downloaded 44 times

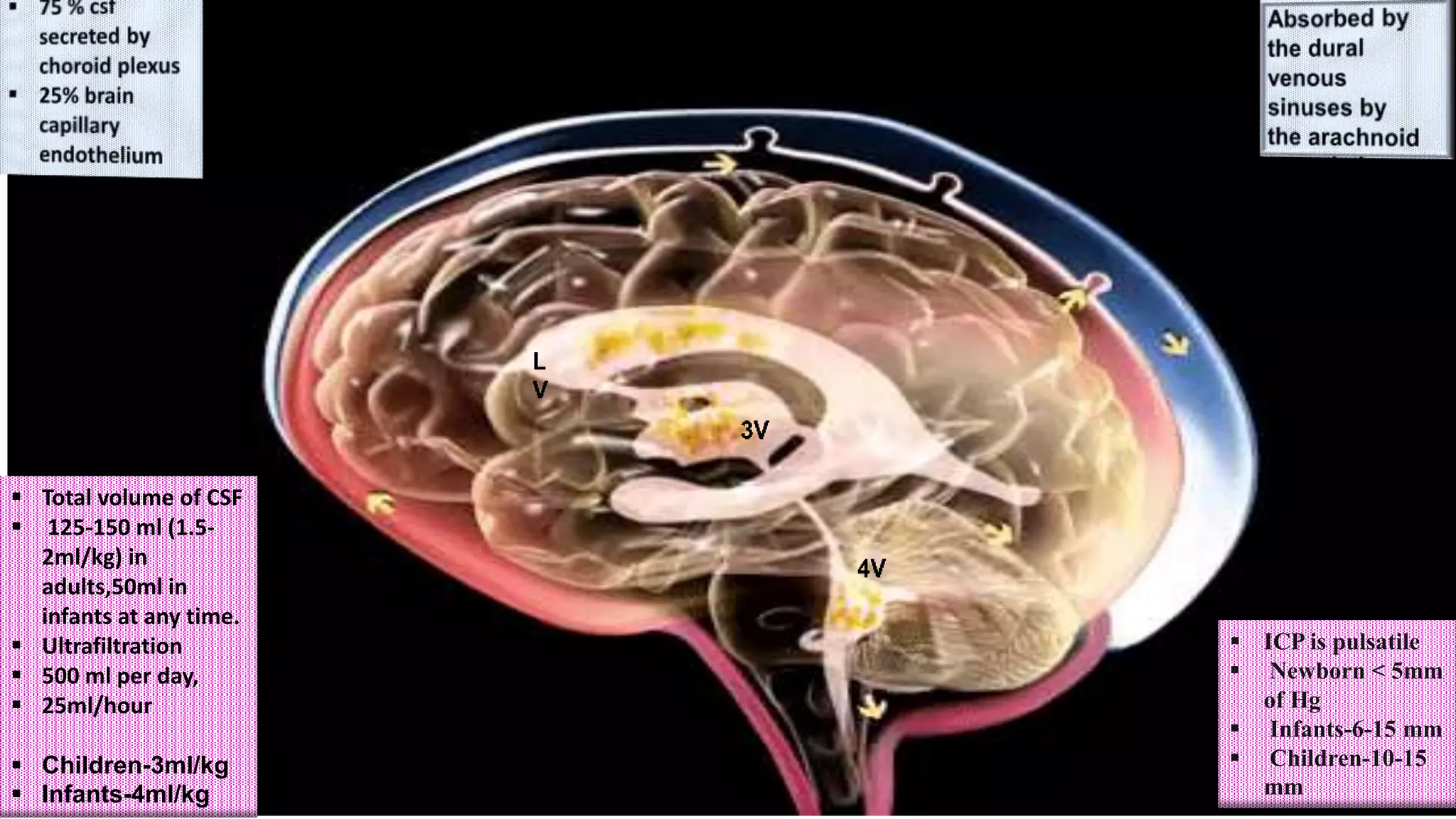



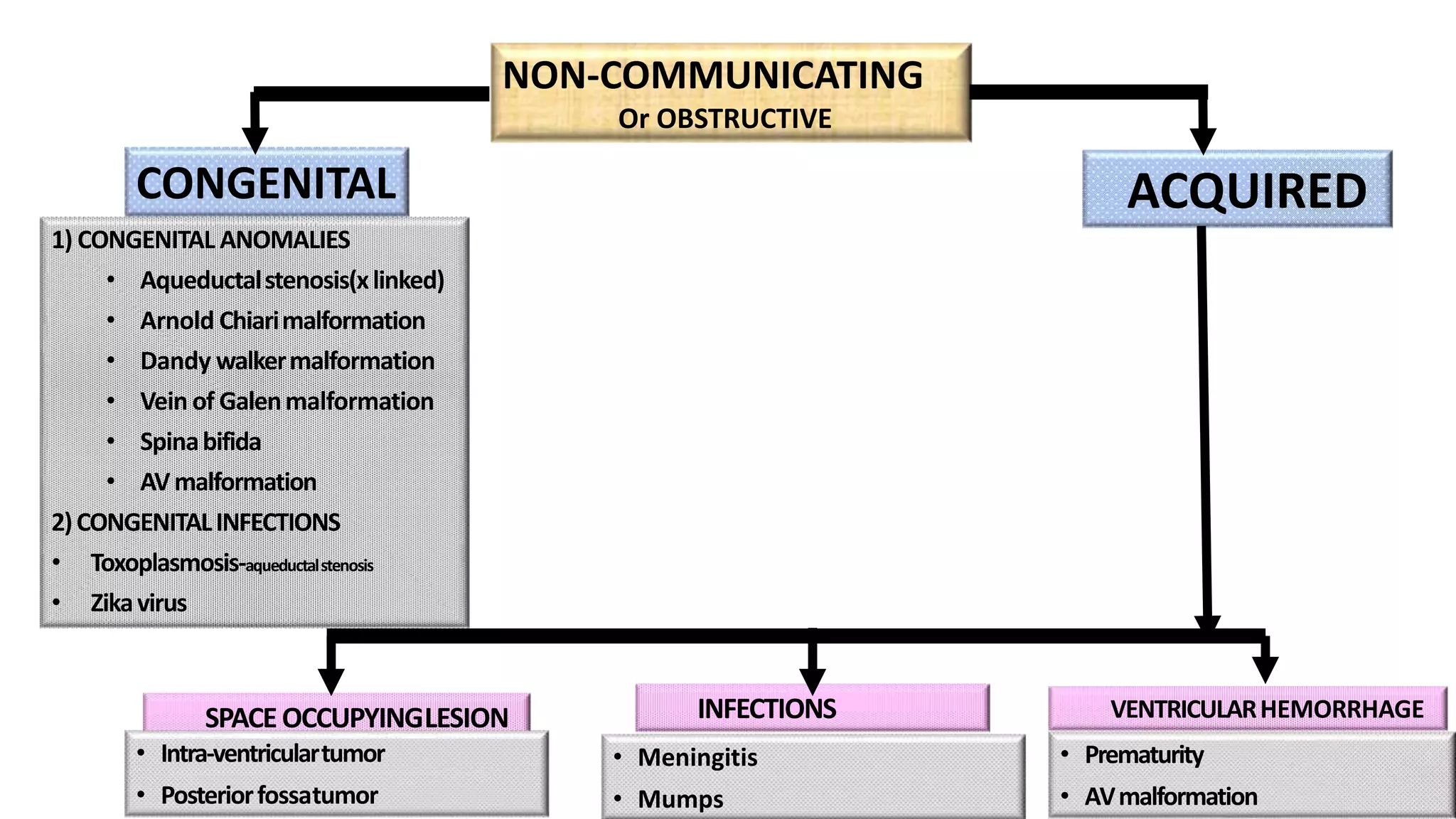
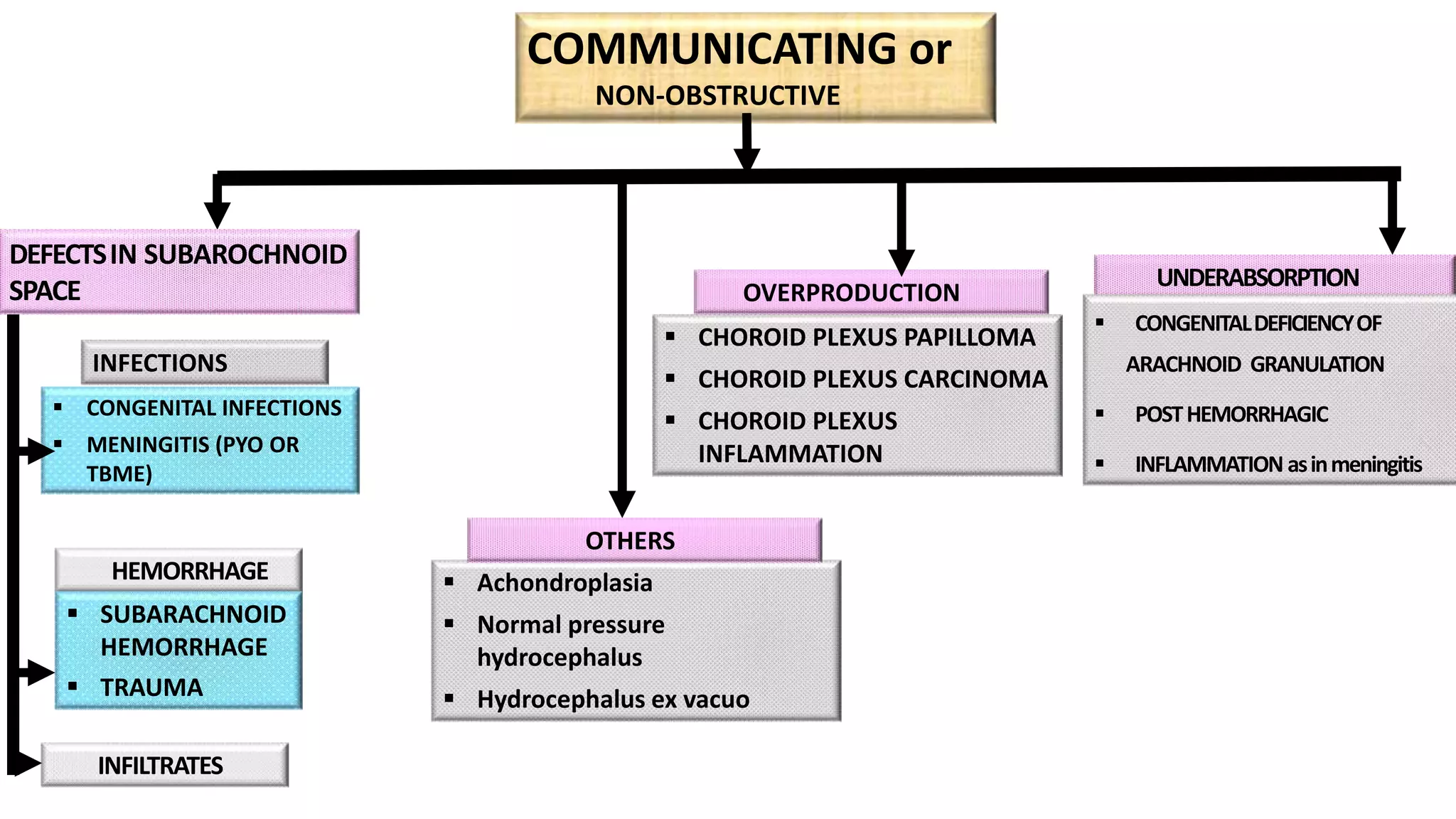

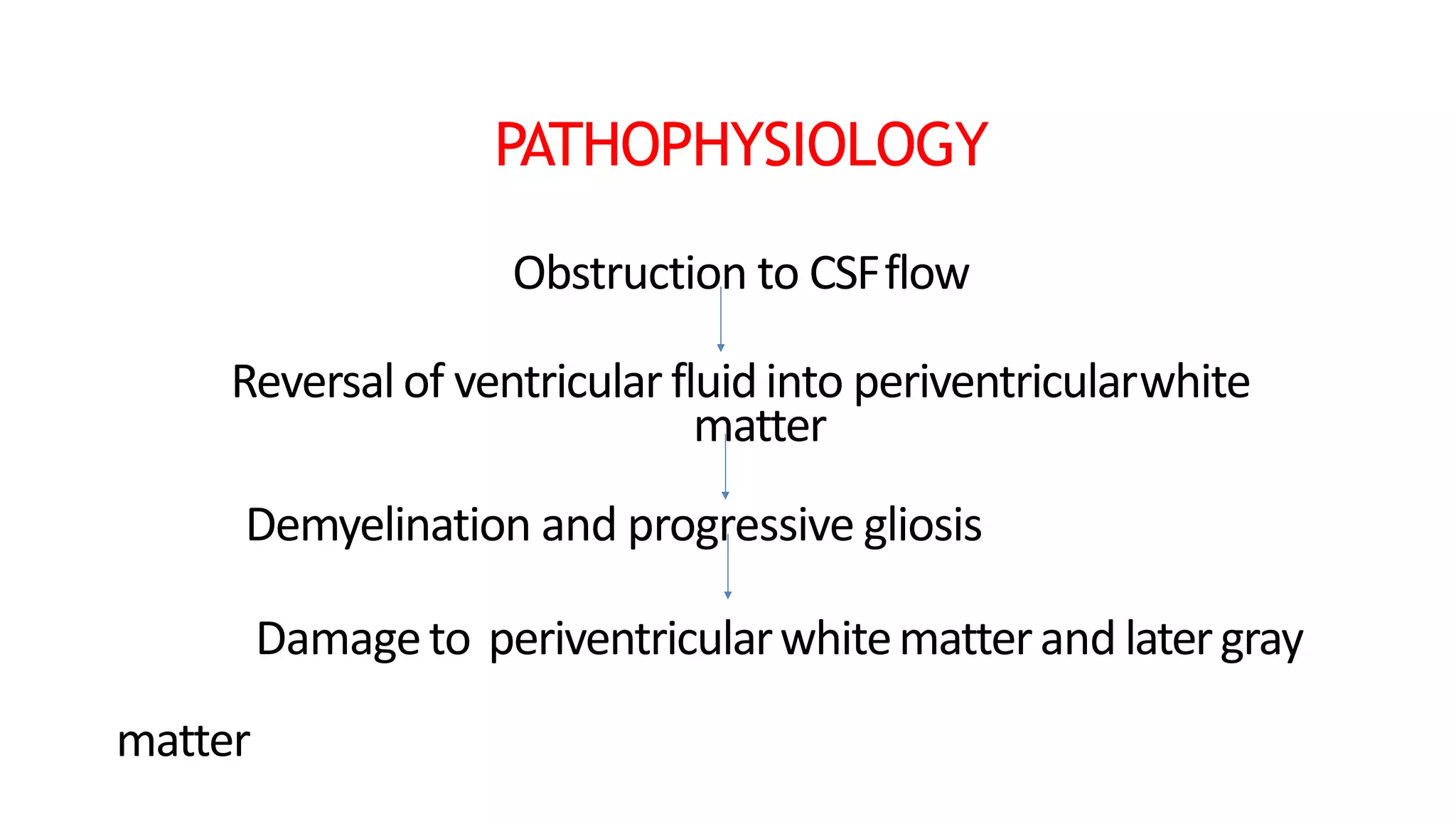






















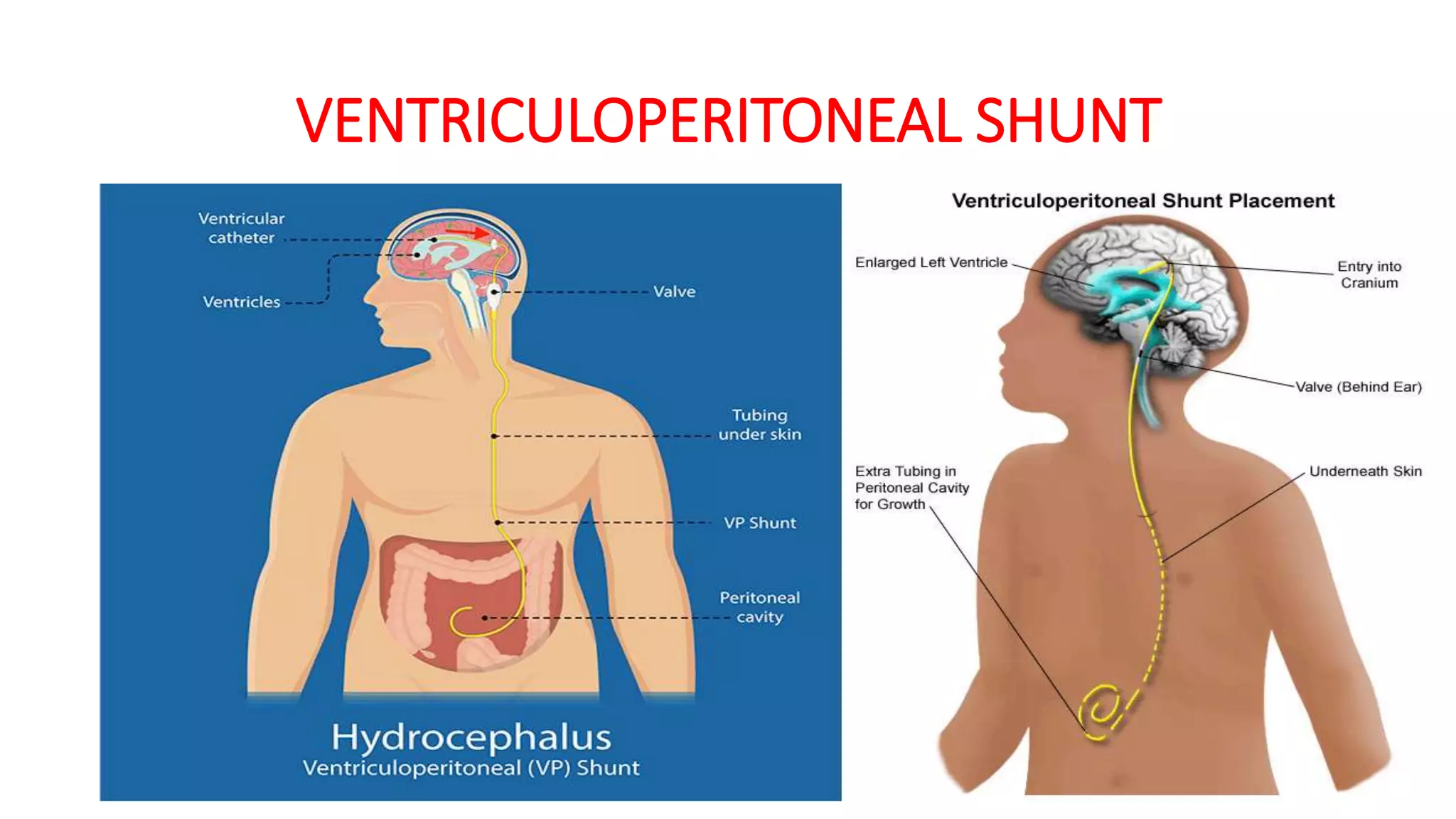






This document discusses hydrocephalus, including: 1) It defines hydrocephalus as an increased volume of cerebrospinal fluid in the ventricles due to overproduction or impaired absorption, causing increased pressure in the skull. 2) There are two main types - communicating/non-obstructive which involves overproduction or underabsorption of CSF, and non-communicating/obstructive which involves obstruction of CSF flow. 3) Clinical features vary depending on age but include increasing head size, irritability, vomiting, and signs of increased intracranial pressure like headache. 4) Treatment involves reducing CSF production medically or surgically placing a shunt to divert CSF out of
























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
















