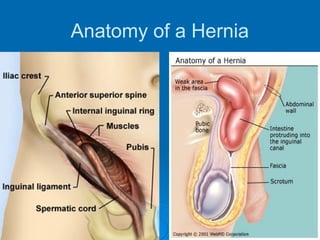
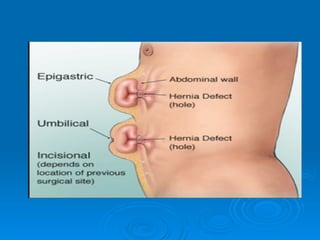
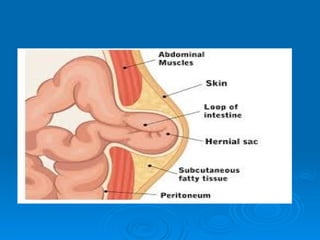
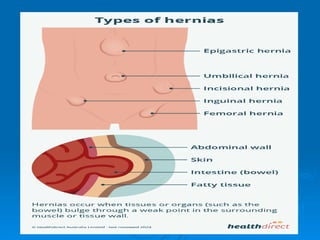
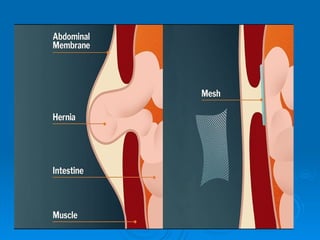
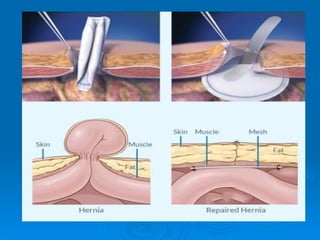
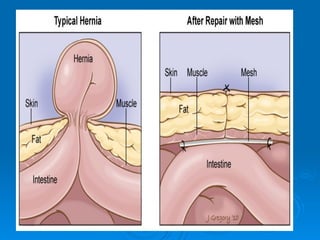
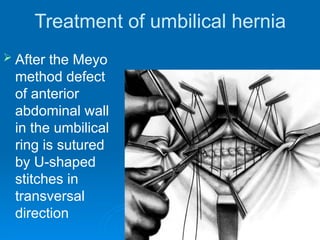
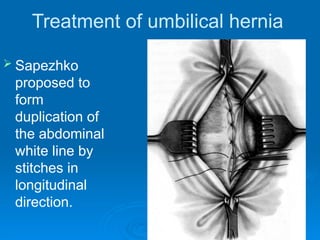
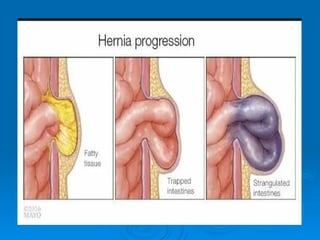
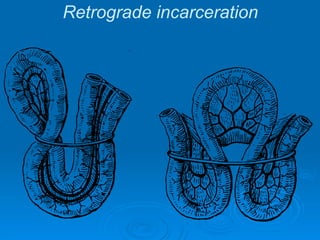
Hernia refers to the bulging of abdominal contents through a weakness in the abdominal wall, with types including external and internal hernias. Diagnosis typically involves physical examination, imaging techniques, and careful observation of symptoms, while management principles focus on reducing the hernia, excising non-viable tissue, and reinforcing the abdominal wall using sutures or mesh. Treatment may vary based on the hernia type and associated complications, with incarcerated hernias requiring more urgent attention.