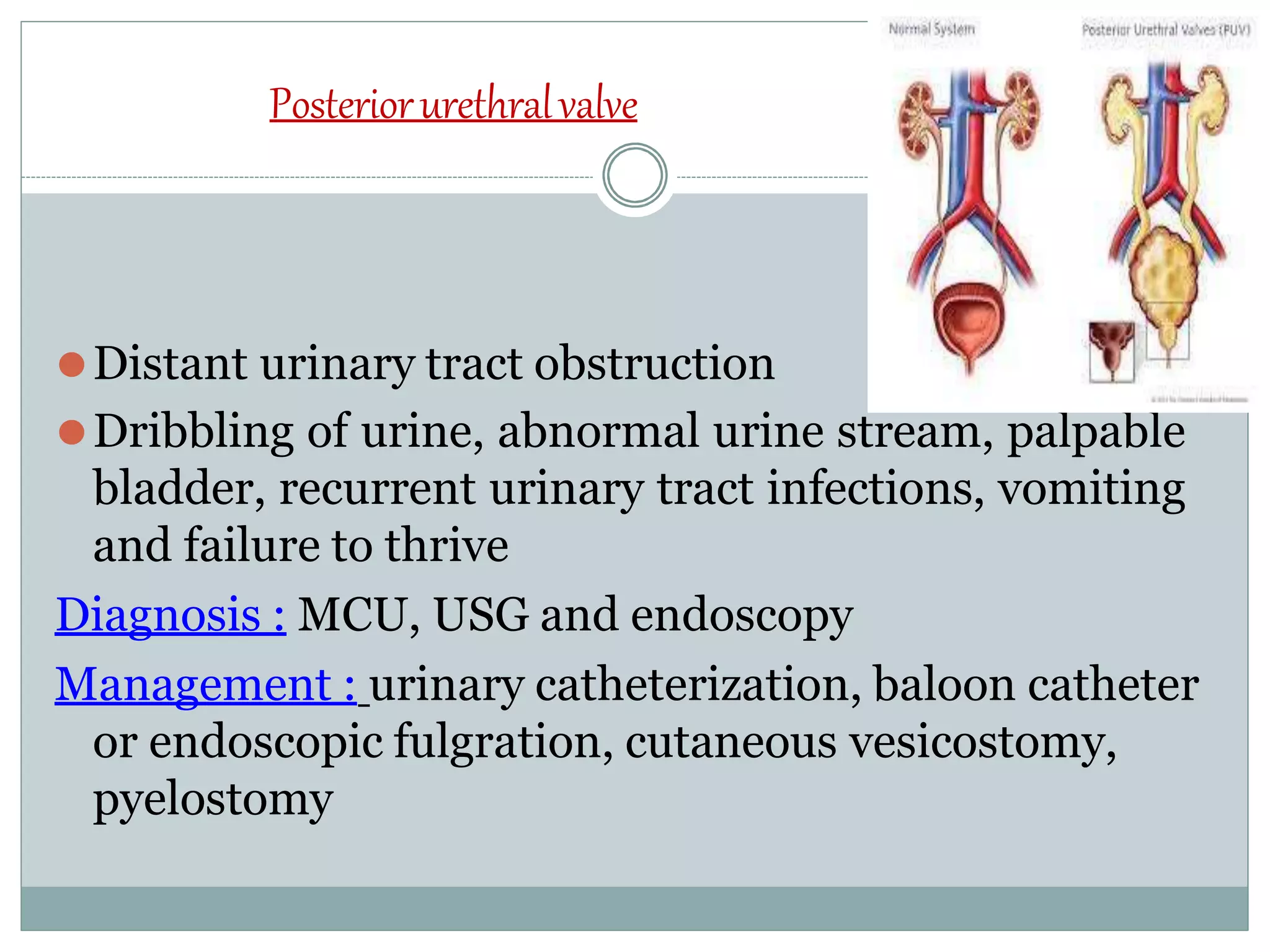
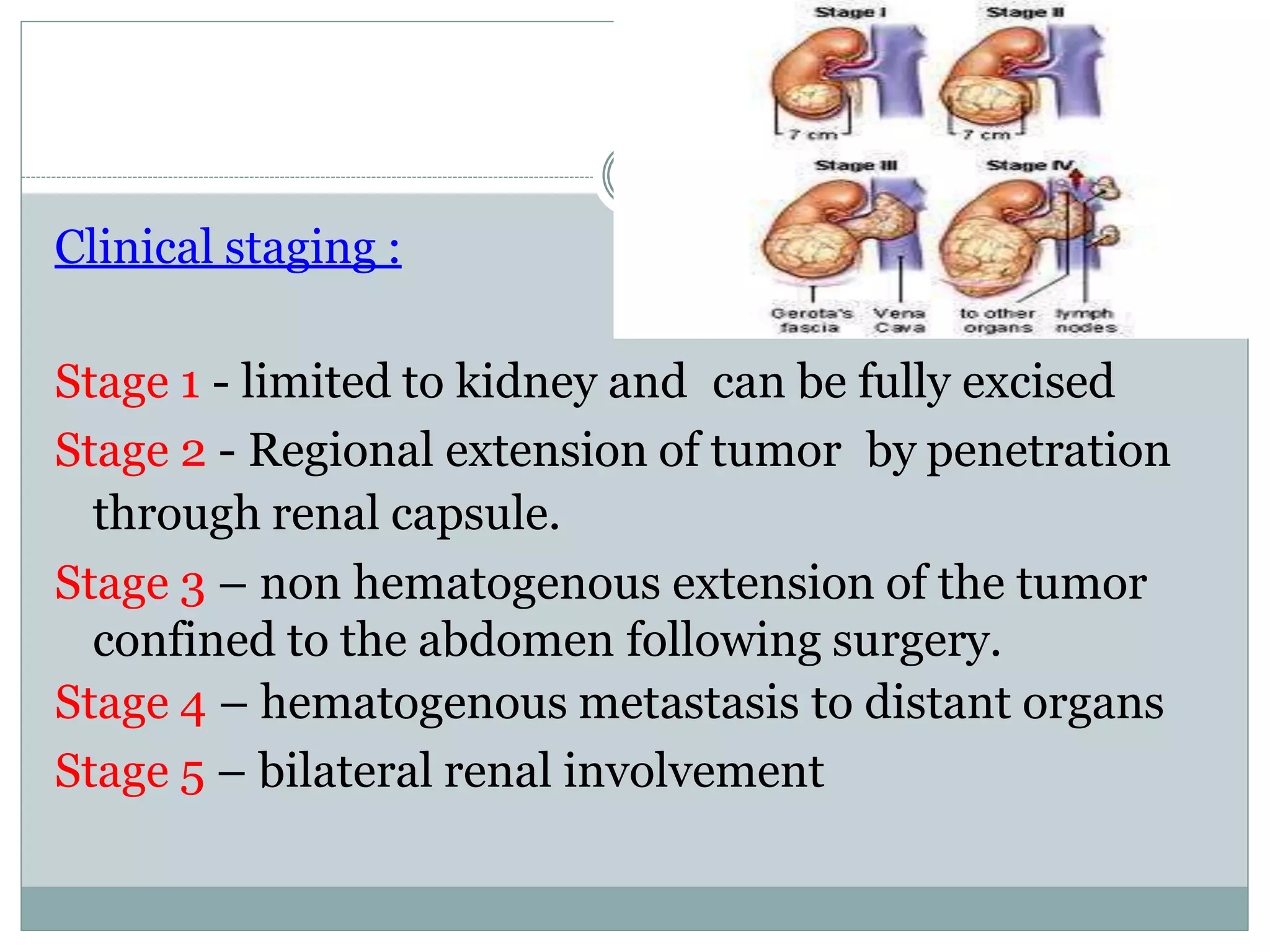
This document discusses congenital genitourinary disorders that commonly affect the kidneys and urinary tract in children. It outlines various abnormalities that can occur in the kidneys, ureters, bladder and urethra. Some of the disorders discussed include renal agenesis, horseshoe kidney, posterior urethral valves, hypospadias, and Wilm's tumor. The document provides details on the symptoms, diagnosis and management of these various congenital genitourinary disorders that can present in pediatric patients.