Downloaded 412 times
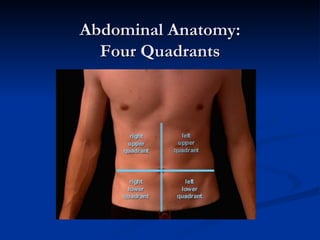
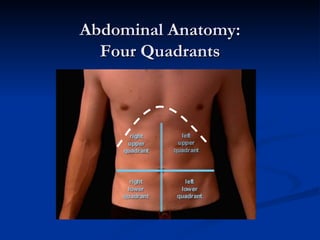
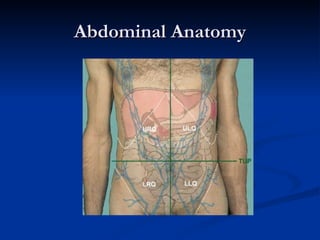

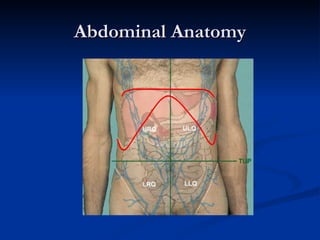
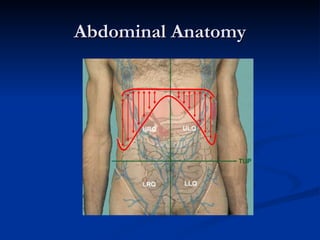
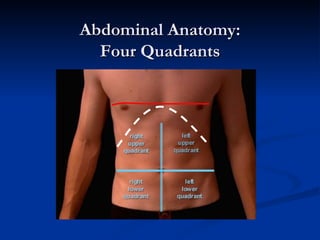
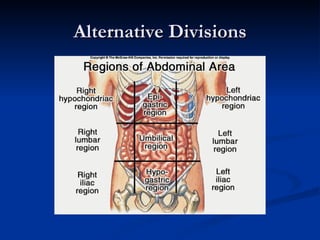
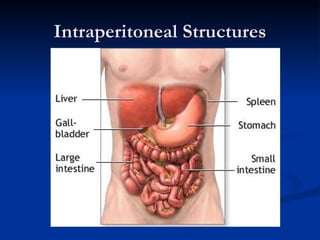
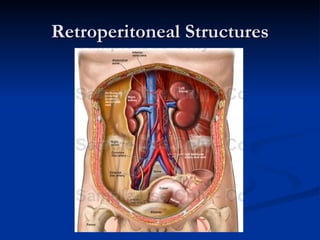
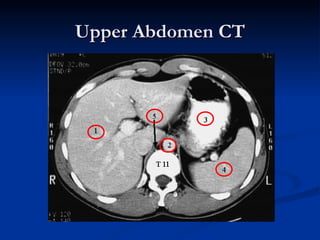
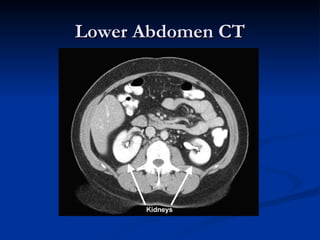
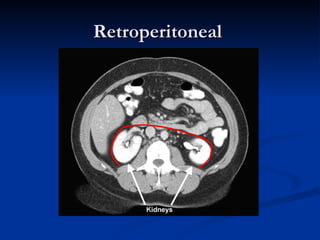
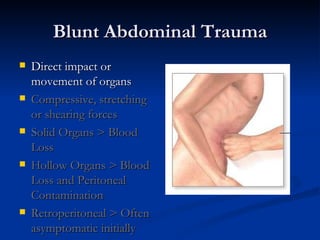
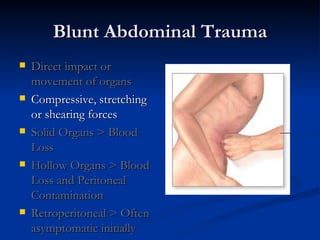
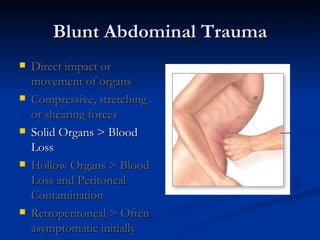
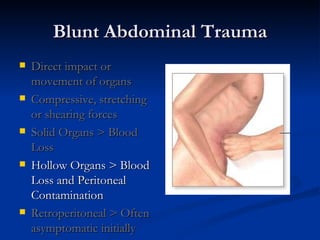
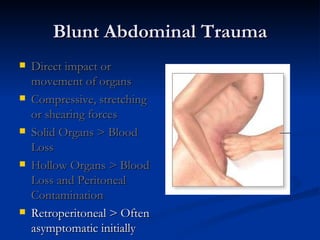



This document summarizes abdominal trauma, including abdominal anatomy, mechanisms of injury, common pathologies, evaluation techniques, and management strategies. It discusses the anatomy of the abdominal organs and potential spaces, mechanisms of blunt versus penetrating trauma, evaluation of solid versus hollow organ injuries, and techniques like physical exam, imaging, and laparotomy. It also reviews injury patterns and management of liver, spleen, and genitourinary trauma.





















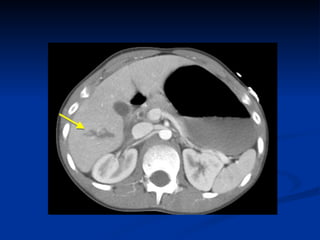
![Spleen[1]](https://cdn.slidesharecdn.com/ss_thumbnails/spleen1-171112094140-thumbnail.jpg?width=640&height=640&fit=bounds)





















































































