Downloaded 15 times
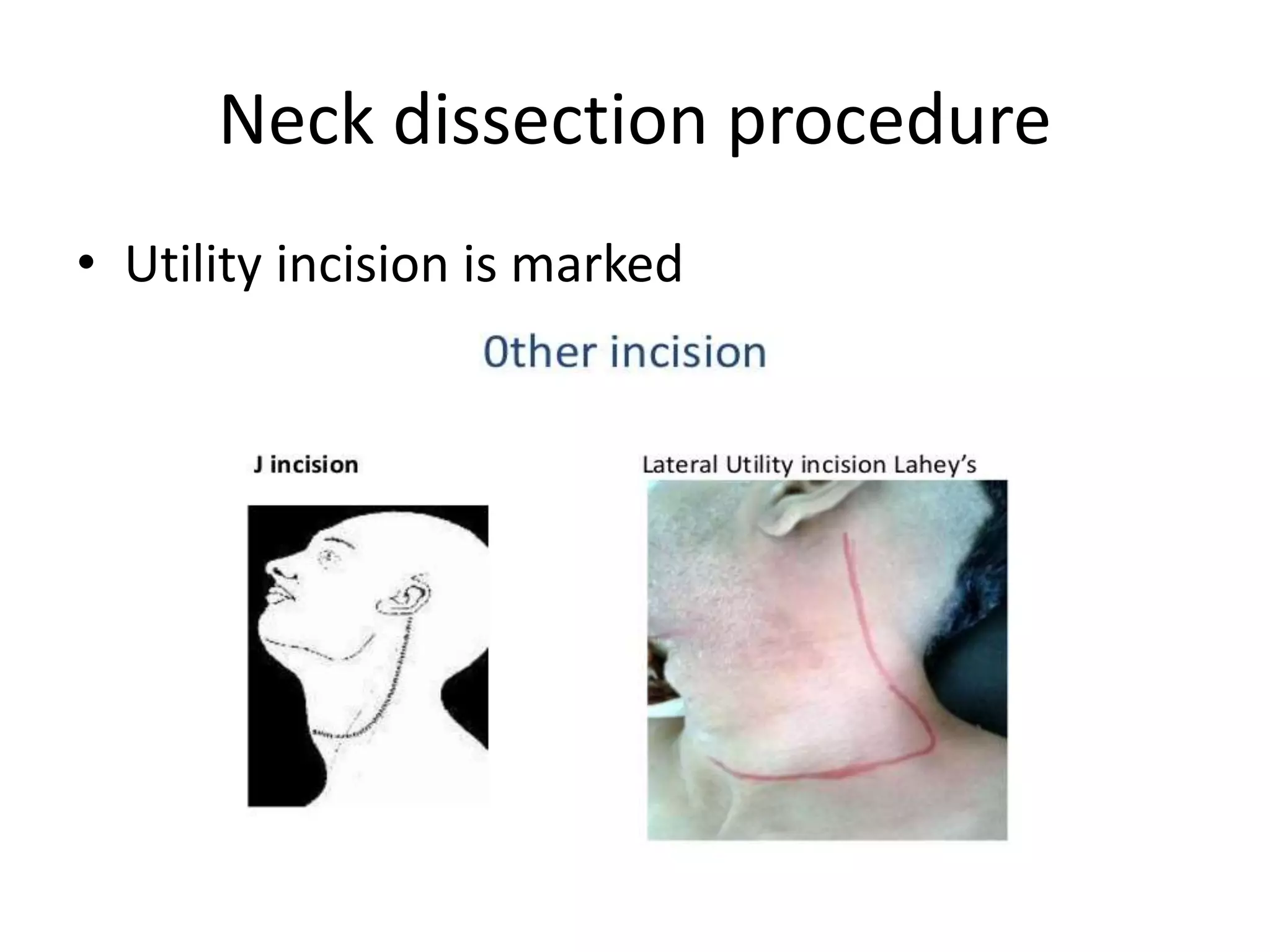

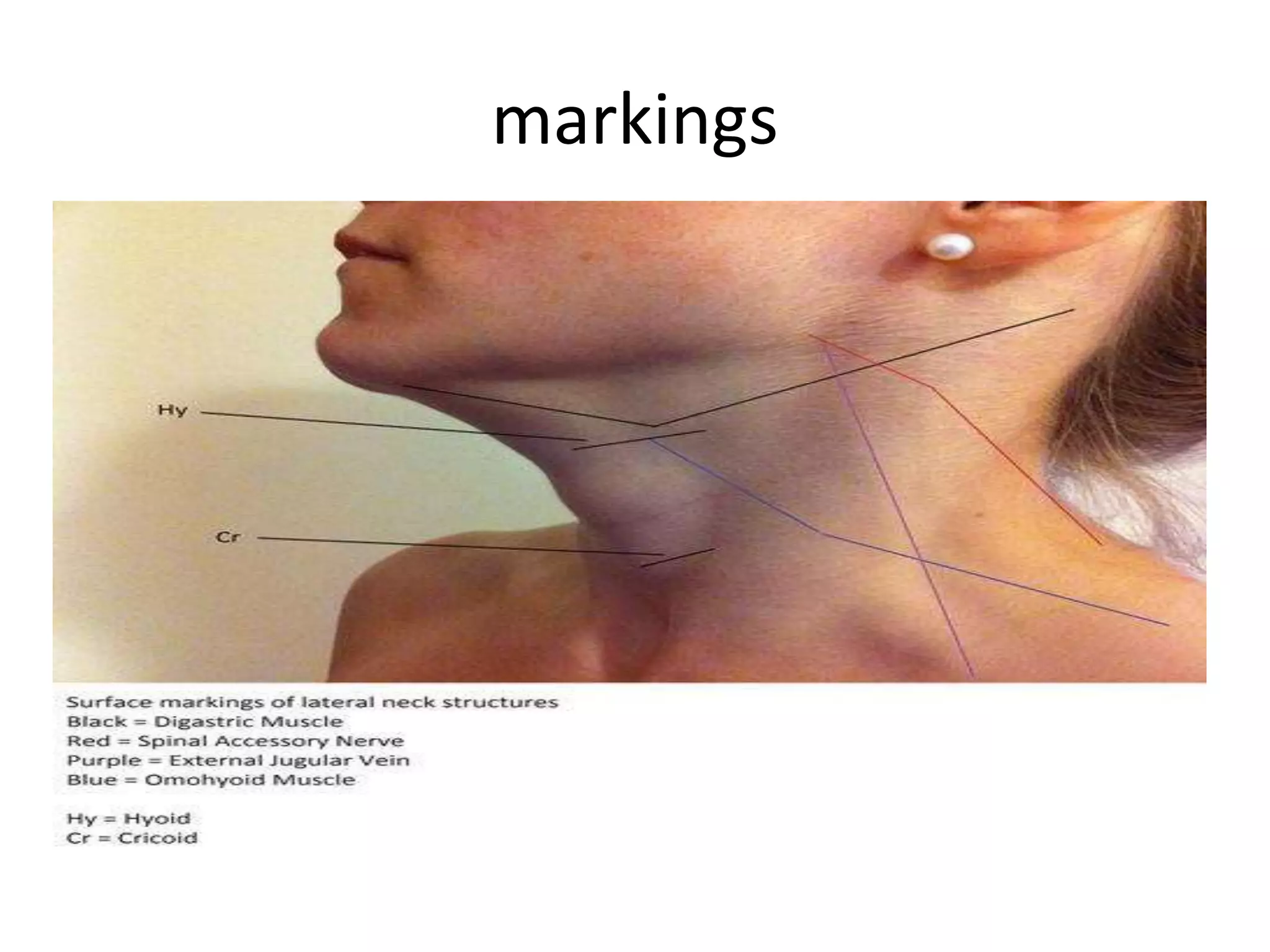















This document describes the procedure for a neck dissection. Key steps include: 1) Making an incision in the neck and elevating subplatysmal flaps to expose the lymph nodes. 2) Dissecting lymph nodes from levels I-V in the neck, moving from superior to inferior levels. Care is taken to avoid important structures like nerves and veins. 3) The entire specimen containing the dissected lymph nodes is delivered from the neck. The wound is then closed.























































































