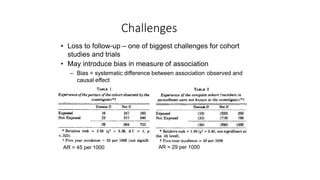
This document outlines the strengths and challenges of cohort studies. The strengths include examining multiple health outcomes and exposures over time without binary classifications. Participants can change exposure levels. Exposures are measured before outcomes, allowing assessment of temporality. Challenges include loss to follow-up, expense of repeated data collection, long time to conduct, inefficiency for rare outcomes, reliance on historical data quality, ensuring blind outcome assessment, challenging exposure classification, requiring sufficient population exposure variation, and loss to follow-up potentially introducing bias if associated with outcomes or exposures.