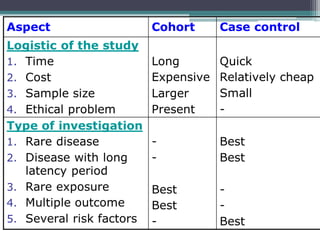
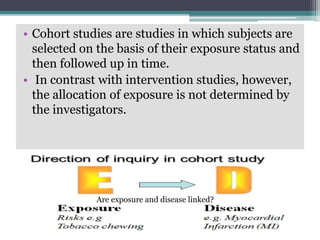
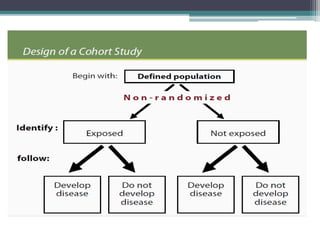
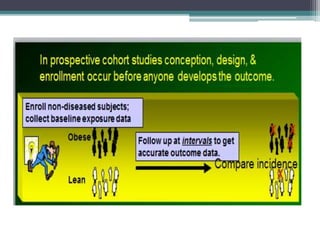
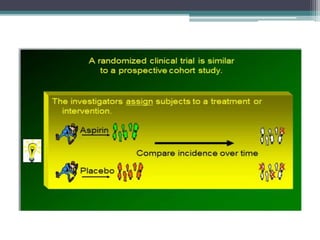
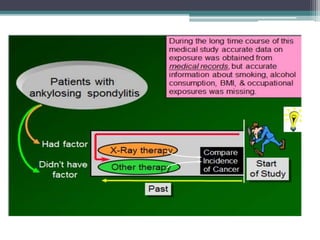
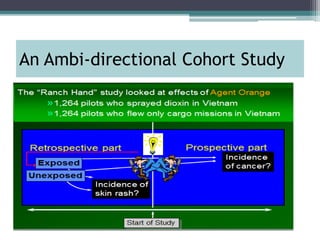
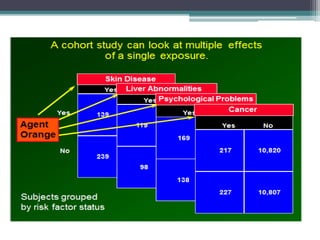
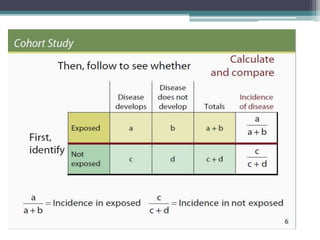
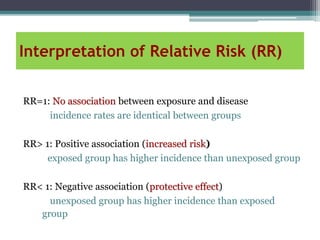
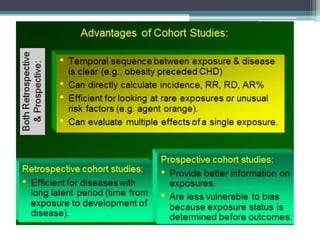
A cohort study involves following groups of individuals over time to examine exposure and disease status. Cohort studies compare disease incidence between exposed and unexposed groups. Key aspects include selecting cohorts based on exposure status, obtaining exposure data, following cohorts over time to measure disease outcomes, and analyzing results by calculating incidence rates and relative risks. Advantages are the ability to establish temporal relationships and measure multiple outcomes, while disadvantages include time and cost requirements and potential for loss to follow-up.