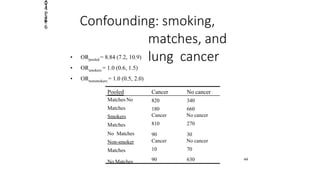
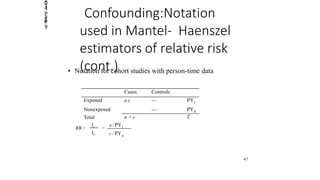
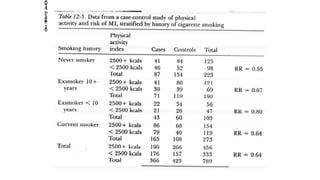
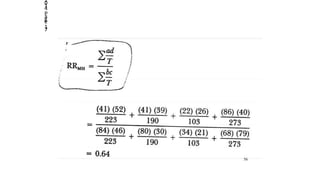
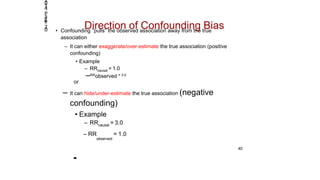
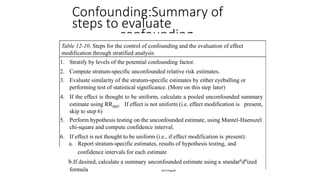
Stratification and multivariate analysis are methods used in epidemiologic studies to reduce confounding. Stratification involves dividing the data into subgroups based on potential confounding variables, and examining the relationship between exposure and outcome separately within each subgroup. The Mantel-Haenszel method provides a pooled estimate that averages the stratum-specific estimates to provide an overall effect estimate adjusted for confounding. Evaluating differences between adjusted and non-adjusted estimates helps determine if confounding is present.