Downloaded 127 times
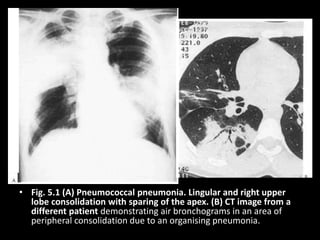
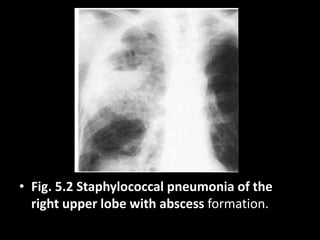
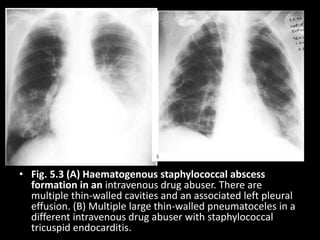
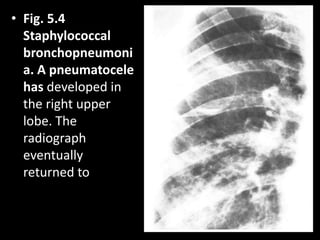
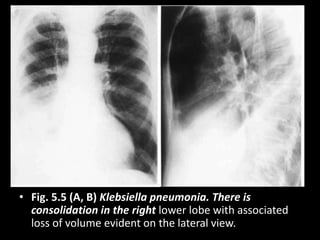
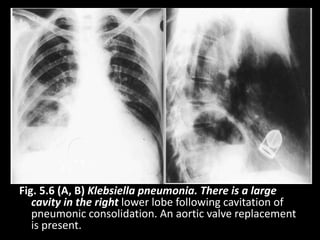
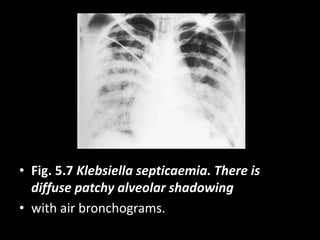
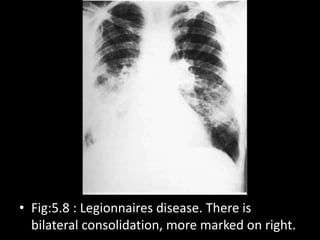
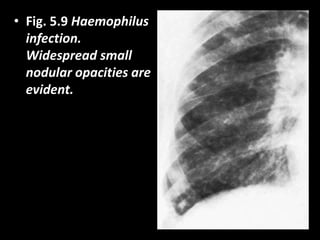
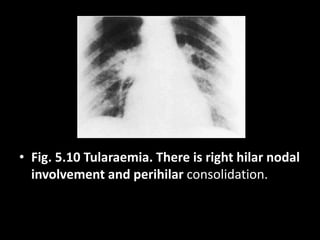
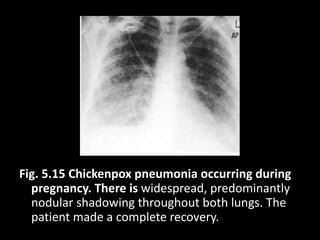
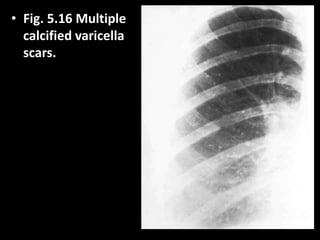
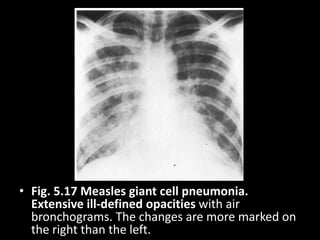
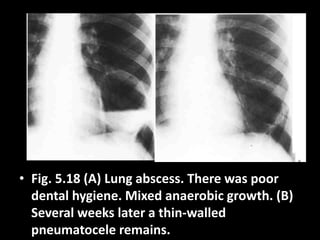
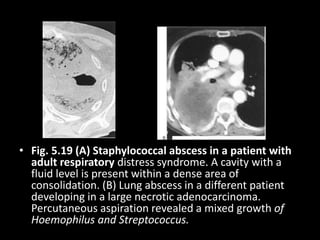
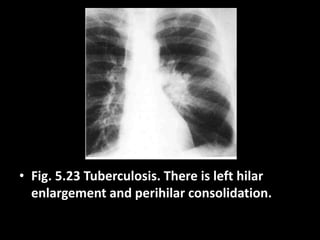
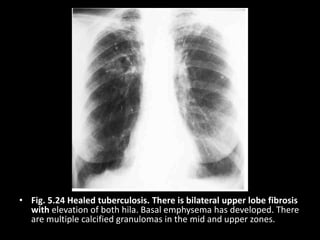
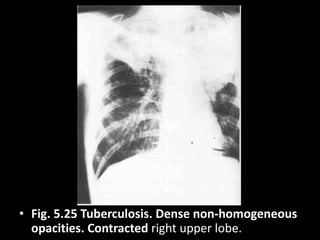
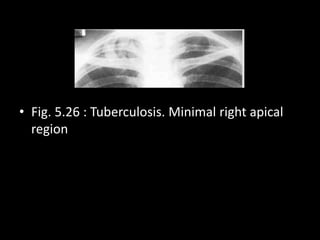
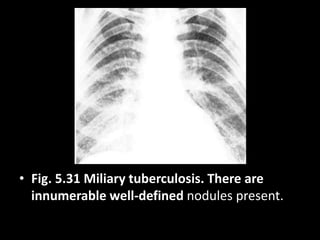
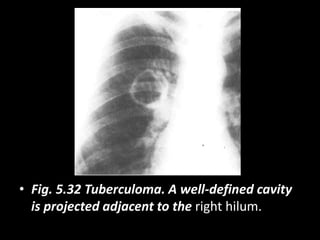
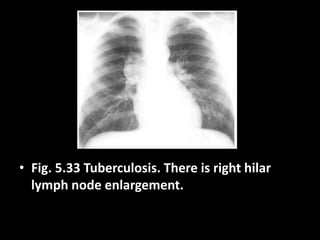
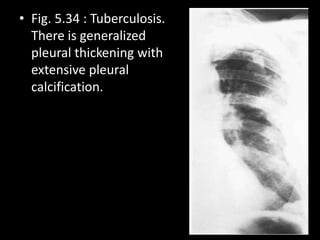
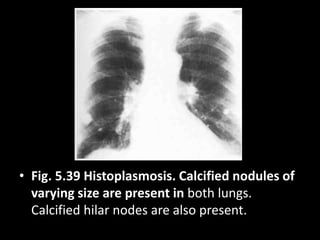
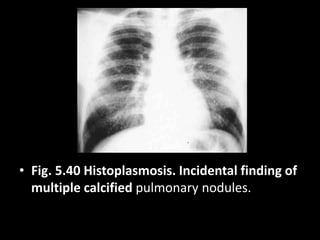
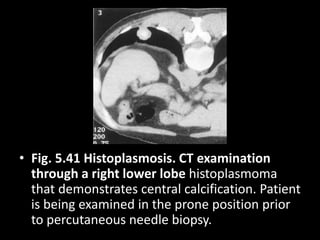
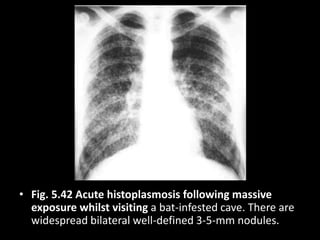
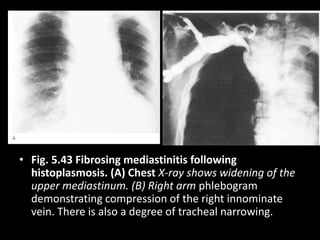
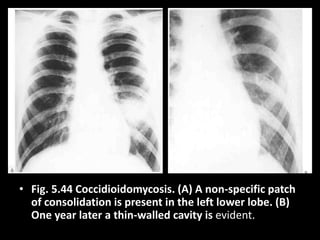
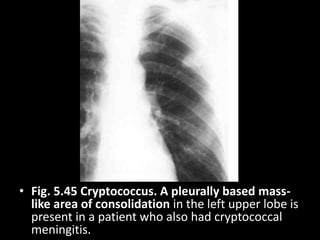
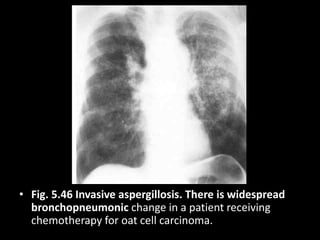
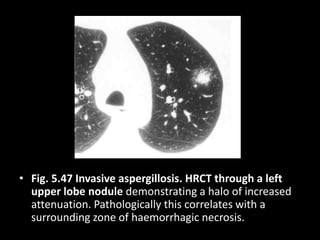
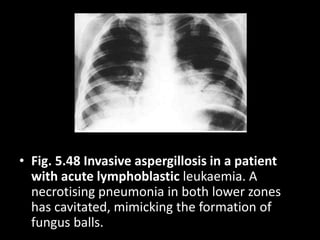
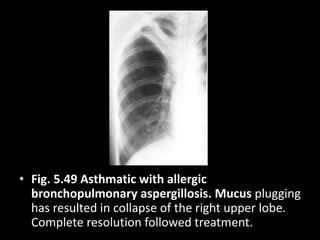
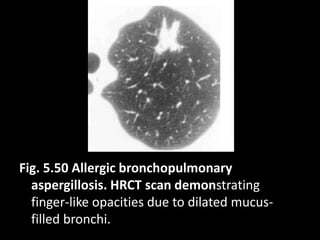
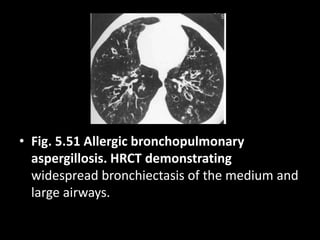
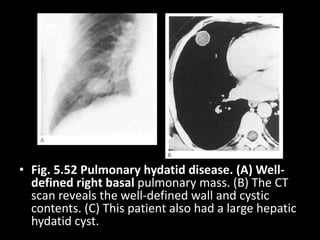
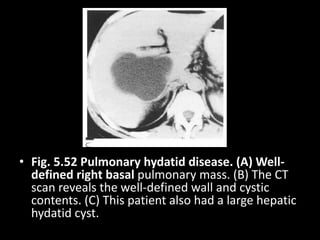
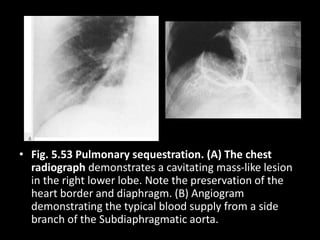
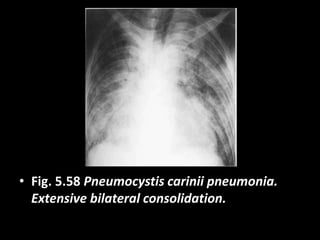
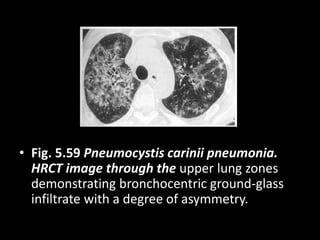
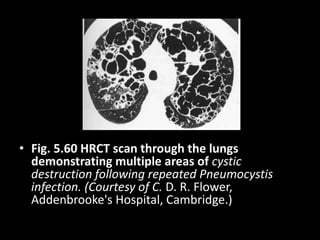
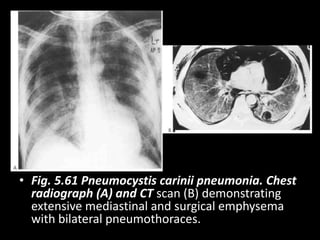
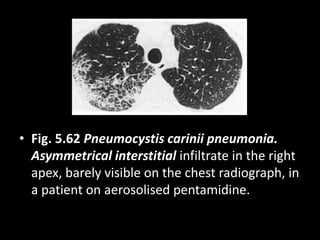
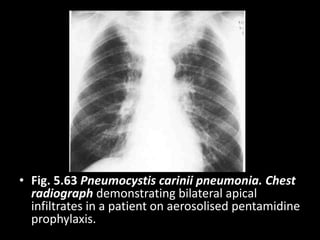
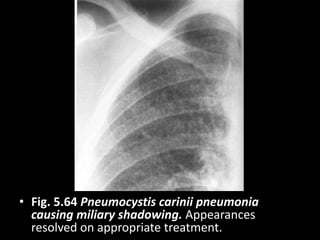
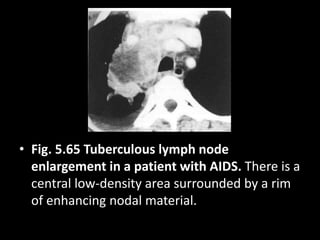
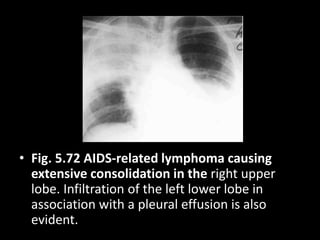

This document contains 72 figures showing various pulmonary infections on chest radiographs and CT scans. The infections included are pneumococcal pneumonia, staphylococcal pneumonia and abscesses, Klebsiella pneumonia, Legionnaires disease, tuberculosis, histoplasmosis, aspergillosis, Pneumocystis pneumonia, and several others. Each figure is labeled with the specific infection and findings on the images.





















































![Chest x ray interpretation of infections [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/chestxrayinterpretationofinfectionsautosaved-200717071240-thumbnail.jpg?width=640&height=640&fit=bounds)








































