
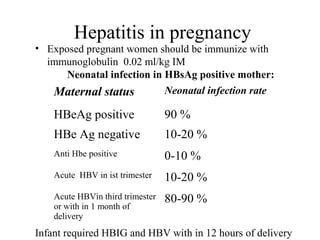


This document discusses various infectious diseases that can affect pregnancy, including their risks, screening recommendations, and treatment/management approaches. For HIV in pregnancy, screening and treatment can reduce transmission risk to the baby to 7.2%. Hepatitis B screening and immunoglobulin treatment within 12 hours of birth can reduce neonatal infection rates. Several infections including parvovirus, rubella, toxoplasmosis, varicella, CMV and listeria can cause fetal complications if acquired during pregnancy. Group B streptococcus is a leading cause of neonatal sepsis, and prenatal screening and intrapartum antibiotics can help prevent transmission.