The document discusses anticoagulants, substances that prevent blood coagulation, their mechanisms, classifications, and therapeutic uses. It details drugs like heparin and warfarin, including their actions, pharmacokinetics, adverse effects, and contraindications. It highlights the importance of anticoagulants in preventing thrombus formation and related conditions.



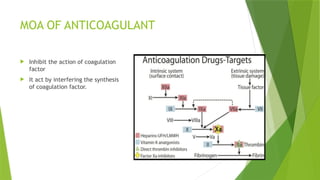




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


