3.Ischemic heart disease( coronary artery disease)
•Download as PPT, PDF•
14 likes•625 views

Ischemic heart disease( coronary artery disease)

Recommended
More Related Content
What's hot
What's hot (20)
Similar to 3.Ischemic heart disease( coronary artery disease)
Similar to 3.Ischemic heart disease( coronary artery disease) (20)
More from PNK SINGH
More from PNK SINGH (20)
Recently uploaded
Recently uploaded (20)
3.Ischemic heart disease( coronary artery disease)
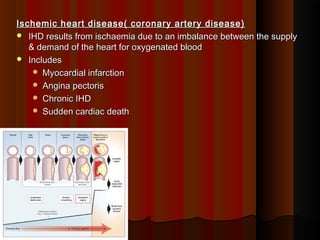
- 1. Ischemic heart disease( coronary artery disease)Ischemic heart disease( coronary artery disease) IHD results from ischaemia due to an imbalance between the supplyIHD results from ischaemia due to an imbalance between the supply & demand of the heart for oxygenated blood& demand of the heart for oxygenated blood IncludesIncludes Myocardial infarctionMyocardial infarction Angina pectorisAngina pectoris Chronic IHDChronic IHD Sudden cardiac deathSudden cardiac death
- 2. Risk factorsRisk factors Non modifiable risk factors:Non modifiable risk factors: AgeAge SexSex Genetics and familial predispositionGenetics and familial predisposition Modifiable risk factors:Modifiable risk factors: SmokingSmoking Heavy drinkingHeavy drinking Diabetes mellitusDiabetes mellitus Hypercholesterolemia and hyperlipidemiaHypercholesterolemia and hyperlipidemia HypertensionHypertension Obesity and sedentary lifestyleObesity and sedentary lifestyle StressStress
- 3. PathogenesisPathogenesis Due to atherosclerosisDue to atherosclerosis 1.1. Atherosclerosis having fixed stenosis plaqueAtherosclerosis having fixed stenosis plaque 90% of cases of IHD have Atherosclerosis90% of cases of IHD have Atherosclerosis 2.2. Acute change in the atherosclerotic plaqueAcute change in the atherosclerotic plaque Rupture, fissuring, ulceration or intraplaque hemorrhageRupture, fissuring, ulceration or intraplaque hemorrhage 3.3. Coronary thrombosisCoronary thrombosis Rupture of atherosclerotic plaque exposes sub endothelial collagen &Rupture of atherosclerotic plaque exposes sub endothelial collagen & may lead to Platelet adherence, activation & autocatalytic chainmay lead to Platelet adherence, activation & autocatalytic chain reaction leading to the formation of thrombusreaction leading to the formation of thrombus 4.4. Coronary Vasospasm or vasoconstrictionCoronary Vasospasm or vasoconstriction
- 4. OthersOthers 5. Nonatherosclerotic coronary disease5. Nonatherosclerotic coronary disease Disorders when involving coronary arteries reduces perfusionDisorders when involving coronary arteries reduces perfusion Emboli to coronary arteriesEmboli to coronary arteries ArteritisArteritis Coccaine abuseCoccaine abuse Trauma to coronary arteriesTrauma to coronary arteries 6. Hemodynamic derangements6. Hemodynamic derangements Hypotension – shock, massive hemorrhage, spinal anesthesiaHypotension – shock, massive hemorrhage, spinal anesthesia Left sided heart failureLeft sided heart failure Increase myocardial demand – tachycardia, hypertrophyIncrease myocardial demand – tachycardia, hypertrophy Reduced oxygen carrying capacity of bloodReduced oxygen carrying capacity of blood
- 5. Coronary Artery DistributionCoronary Artery Distribution LAD (40-50%) - anterior wall LV, apex, anterior IV septumLAD (40-50%) - anterior wall LV, apex, anterior IV septum Right (30-40%) - posterior wall LV, posterior IV septumRight (30-40%) - posterior wall LV, posterior IV septum Left circumflex (15-20%) - lateral wall LVLeft circumflex (15-20%) - lateral wall LV
- 6. ANGINA PECTORISANGINA PECTORIS It is characterized by paroxysmal and usually recurrent attacks ofIt is characterized by paroxysmal and usually recurrent attacks of substernal or precordial chest discomfort or pain caused bysubsternal or precordial chest discomfort or pain caused by transient (15 seconds to 15 minutes) myocardial ischemia.transient (15 seconds to 15 minutes) myocardial ischemia. There is a sense of oppression or tightness in the chest like a bandThere is a sense of oppression or tightness in the chest like a band round the chest or feeling of choking occursround the chest or feeling of choking occurs Sometimes in the left jaw,neck, shoulder, arm & handSometimes in the left jaw,neck, shoulder, arm & hand
- 7. There are three overlappingThere are three overlapping patterns of anginapatterns of angina pectoris:pectoris: (1) Stable or typical angina,(1) Stable or typical angina, (2) Prinzmetal or variant angina, and(2) Prinzmetal or variant angina, and (3) Unstable or crescendo angina.(3) Unstable or crescendo angina. Some ischemic heart disease are not perceived by patients, evenSome ischemic heart disease are not perceived by patients, even though such events may have adverse prognostic implicationsthough such events may have adverse prognostic implications ( silent ischemia).( silent ischemia).
- 8. Stable (typical) anginaStable (typical) angina Caused by the reduction of coronary perfusion by stenosingCaused by the reduction of coronary perfusion by stenosing coronary atherosclerosis to increased demand e.g during physicalcoronary atherosclerosis to increased demand e.g during physical activity, emotional excitement, or any other cause of increasedactivity, emotional excitement, or any other cause of increased cardiac workload.cardiac workload. Caused by coronary artery atherosclerosis with luminal narrowingCaused by coronary artery atherosclerosis with luminal narrowing greater than 75%greater than 75% Chest pain is brought on by increased cardiac demandChest pain is brought on by increased cardiac demand
- 9. Prinzmetal variant anginaPrinzmetal variant angina It is a type of angina caused by coronary arteryIt is a type of angina caused by coronary artery vasospasm.vasospasm. There is episodic chest pain often occurring at rest.There is episodic chest pain often occurring at rest.
- 10. Unstable or crescendo anginaUnstable or crescendo angina Caused by formation of a non occlusive thrombus in an area ofCaused by formation of a non occlusive thrombus in an area of coronary atherosclerosiscoronary atherosclerosis Increasing frequency, intensity, and duration of episodesIncreasing frequency, intensity, and duration of episodes Occurs at rest / less effortOccurs at rest / less effort High risk for myocardial infarction/ preinfarction anginaHigh risk for myocardial infarction/ preinfarction angina
- 11. Myocardial InfarctionMyocardial Infarction Infarction of an area of a heart muscle, usually as a result of occlusionInfarction of an area of a heart muscle, usually as a result of occlusion of coronary arteryof coronary artery Clinically pain is like angina but of more severe intensityClinically pain is like angina but of more severe intensity MI rises progressively with increasing ageMI rises progressively with increasing age Types of MITypes of MI Transmural InfarctTransmural Infarct Subendocardial/ Non transmual infarctSubendocardial/ Non transmual infarct
- 12. 1. Reduction in coronary1. Reduction in coronary blood flowblood flow AtherosclerosisAtherosclerosis Coronary Vasospasm orCoronary Vasospasm or vasoconstrictionvasoconstriction Thrombosis due toThrombosis due to complicated atheromacomplicated atheroma Emboli to coronary arteriesEmboli to coronary arteries ArteritisArteritis Trauma to coronary arteriesTrauma to coronary arteries 3. Availability of oxygen in3. Availability of oxygen in bloodblood Decreased inDecreased in Severe anaemiaSevere anaemia Advanced lung diseaseAdvanced lung disease Carbon monoxide poisoiningCarbon monoxide poisoining Cynotic congenital heart diseseCynotic congenital heart disese 2. Increase myocardial demand2. Increase myocardial demand Tachycardia as occurs in exercise,Tachycardia as occurs in exercise, infection, pregnancy, hyperthyroidisminfection, pregnancy, hyperthyroidism & hypermetabolism& hypermetabolism Hemodynamic derangements asHemodynamic derangements as occurs in Hypotension due to shock,occurs in Hypotension due to shock, massive haemorrage, spinalmassive haemorrage, spinal anesthesia,anesthesia, Tricuspid regurgitation & Left sidedTricuspid regurgitation & Left sided heart failure – hypertrophyheart failure – hypertrophy MI results from imbalanceMI results from imbalance between supply & demand of thebetween supply & demand of the heart for oxygenated bloodheart for oxygenated blood Myocardial InfarctionMyocardial Infarction
- 13. Coronary artery with thrombus
- 14. Transmural InfarctTransmural Infarct Endocardium to epicardium/ full thickness in the distribution ofEndocardium to epicardium/ full thickness in the distribution of involved arteryinvolved artery Usually associated withUsually associated with coronary atherosclerosiscoronary atherosclerosis Acute palque changeAcute palque change Superimposed thrombosisSuperimposed thrombosis Necrosis most likely begins in the subendocardiumNecrosis most likely begins in the subendocardium
- 15. Subendocardial InfarctSubendocardial Infarct This is limited to the inner 1/3This is limited to the inner 1/3rdrd to 1/2 of the ventricular wallto 1/2 of the ventricular wall Associated with diffuse stenosing coronary atherosclerosisAssociated with diffuse stenosing coronary atherosclerosis Not associated with atherosclerotic palque rupture or superimposedNot associated with atherosclerotic palque rupture or superimposed thrombosisthrombosis For this reason this is less dangerousFor this reason this is less dangerous
- 16. ChangesChanges Ischaemic myocardium undergoes progressive biochemical, functional &Ischaemic myocardium undergoes progressive biochemical, functional & morphological changesmorphological changes MorphologyMorphology SiteSite Undergoes progressive sequences of coagulative necrosisUndergoes progressive sequences of coagulative necrosis Necrosis elicits acute inflammation with neutrophils infiltration in 4- 12 hrNecrosis elicits acute inflammation with neutrophils infiltration in 4- 12 hr Later macrophages remove the dead materials most marked in 3-7 daysLater macrophages remove the dead materials most marked in 3-7 days Neovascularisation & proliferation of fibroblast at the margin leads toNeovascularisation & proliferation of fibroblast at the margin leads to fibrous organisationfibrous organisation Finally producing an scarFinally producing an scar
- 17. Light microscopeLight microscope 1.1. Waviness of fibres at bordersWaviness of fibres at borders 2.2. Beginning of coagulation necrosis,Beginning of coagulation necrosis, oedema, haemorrhage, beginoedema, haemorrhage, begin neutrophilic infiltrationneutrophilic infiltration 3.3. Continuing coagulation necrosis,Continuing coagulation necrosis, pallor(pyknosis of nuclei,pallor(pyknosis of nuclei, shrunken eosinophilic cytoplasmshrunken eosinophilic cytoplasm marginal contraction bandmarginal contraction band necrosisnecrosis Gross changeGross change 1.1. -- 2.2. -- 3.3. PallorPallor 4.4. PallorPallor sometimessometimes hyperemiahyperemia Time 1.1-2 hours 2.4-12 hours 3.18-24 hours
- 18. Contraction bands in an early infarct. They are dark pink, and consist of greatly contracted, ineffective actin and myosin fibrils.
- 19. Coagulative necrosis plus many neutrophils (2-3 day old infarct).
- 20. Light microscopeLight microscope 1.1. Total coagulation necrosis withTotal coagulation necrosis with loss of nuclei & striations, heavyloss of nuclei & striations, heavy interistial infiltrate of neutrophilsinteristial infiltrate of neutrophils 2.2. Beginning disintegration of deadBeginning disintegration of dead myofibries & resorption ofmyofibries & resorption of sarcoplasm by macrophages,sarcoplasm by macrophages, onset of marginal fibrovascularonset of marginal fibrovascular responseresponse Gross changeGross change 1.1. PallorPallor sometimessometimes hyperemiahyperemia 2.2. HyperemicHyperemic border,border, central yellowcentral yellow brownbrown softeningsoftening 3.3. Time 1.24 - 72hours 2.3-7 days
- 21. Infarct with numerous macrophages (slightly older, ~7 days).
- 22. Light microscopeLight microscope 1.1. Well developedWell developed phagocytosis, prominentphagocytosis, prominent granulation tissue withgranulation tissue with fibrovascular reaction infibrovascular reaction in marginmargin 2.2. -- Gross changeGross change 1.1. Maximally yellow 7Maximally yellow 7 soft, vascularisedsoft, vascularised margins, red-brownmargins, red-brown & depressed& depressed 2.2. Scarring completeScarring complete Time 1.10 days 2.7th week
- 23. Macrophages and granulation tissue (~ 10-day-old infarct)
- 24. Pale area in recent infarct
- 25. Old infarct. It is a firm scar
- 26. MI - ComplicationsMI - Complications ArrhythmiasArrhythmias Commonest cause of death is ventricular arrhythmia, usuallyCommonest cause of death is ventricular arrhythmia, usually within the first hourwithin the first hour CHF and pulmonary edemaCHF and pulmonary edema Cardiogenic shockCardiogenic shock Pericarditis and pneumonitis( Dressler’s syndrome)Pericarditis and pneumonitis( Dressler’s syndrome) Mural thrombosisMural thrombosis Rupture of papillary muscle causing acute mitral insufficiency( day 3)Rupture of papillary muscle causing acute mitral insufficiency( day 3)
- 27. MI - ComplicationsMI - Complications Rupture of ventricular wall causing cardiac tamponade( day 4-7)Rupture of ventricular wall causing cardiac tamponade( day 4-7) Rupture of ventricular septum causing VSDRupture of ventricular septum causing VSD Ventricular aneurysmVentricular aneurysm
- 28. Recent infarct with perforation
- 29. Recent infarct with huge mural thrombus
- 30. Chronic Ischemic Heart DiseaseChronic Ischemic Heart Disease Is cardiac muscle insufficiency due to ischaemic myocardial damageIs cardiac muscle insufficiency due to ischaemic myocardial damage leading to slow progressive heart failureleading to slow progressive heart failure Replacement of myocardial fibers by fibrous tissue which tends toReplacement of myocardial fibers by fibrous tissue which tends to be progressivebe progressive Compensatory hypertrophy of non- infarcted musclesCompensatory hypertrophy of non- infarcted muscles 40% of mortality in IHD40% of mortality in IHD Ischemic cardiomyopathyIschemic cardiomyopathy
- 31. Diffuse fibrosis in chronic ischemic heart disease. There is also myocyte hypertrophy and a decrease in small vessels.
- 33. Sudden cardiac death o Definition: death within 1 hour of cardiac events Etiology o In the vast majority of cases in adults, sudden cardiac death is a complication and often the first clinical manifestation of IHD. oMechanism: fatal cardiac arrhythmia; usually ventricular fibrillation Common causes are: o Coronary artery disease (80%) o Hypertrophic cardiomyopathy o Mitral valve prolapse o Aortic valve stenosis o Congenital heart abnormalities o Myocarditis
- 34. Diffuse fibrosis in chronic ischemic heart disease. There is also myocyte hypertrophy and a decrease in small vessels.
- 35. Lab diagnosis of MILab diagnosis of MI HistoryHistory ECGECG Routine blood examinationsRoutine blood examinations Neutrophil leucocytosisNeutrophil leucocytosis ESR raisedESR raised Estimation of serum enzymeEstimation of serum enzyme
- 36. ECG change seen in MIECG change seen in MI - ST segment elevation- ST segment elevation - Abnormal Q waves representing myocardial necrosis develop in 24- Abnormal Q waves representing myocardial necrosis develop in 24 to 48 hrsto 48 hrs - Inverted T wave- Inverted T wave
- 37. Cardiac enzymes with their time of riseCardiac enzymes with their time of rise
- 38. What are the risk factors for atherosclerosis / IHDWhat are the risk factors for atherosclerosis / IHD What are the complications of atherosclerosisWhat are the complications of atherosclerosis Give the morphology of atherosclerosisGive the morphology of atherosclerosis Give the pathogenesis of atherosclerosisGive the pathogenesis of atherosclerosis Define IHD. Classify IHDDefine IHD. Classify IHD What are the complications/fates of IHDWhat are the complications/fates of IHD Describe the pathogenesis of MIDescribe the pathogenesis of MI Give the lab diagnosis of MIGive the lab diagnosis of MI What are the sequences of changes / morphology of MIWhat are the sequences of changes / morphology of MI