Download to read offline

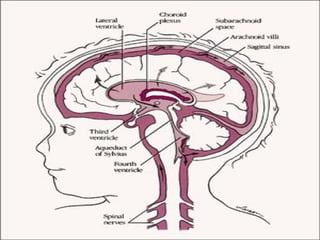
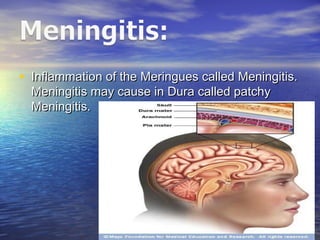



The document discusses hydrocephalus and meningitis. It defines hydrocephalus as increased cerebrospinal fluid (CSF) within the skull accompanied by ventricle dilation and increased intracranial pressure. Hydrocephalus is classified as internal, involving ventricle dilation, or external, with CSF collection in the subarachnoid space. CSF is produced by the choroid plexus and circulates through the ventricles before being absorbed into blood vessels. Hydrocephalus can be primary, due to CSF overproduction, obstruction, or deficient absorption, or secondary, from neural tissue loss without pressure rise. Meningitis refers to the inflammation of the meninges covering the brain and spinal cord. It discusses























































































