Download to read offline



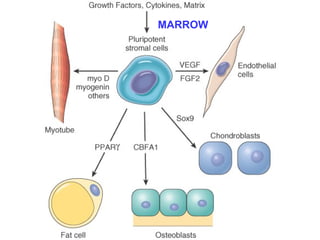
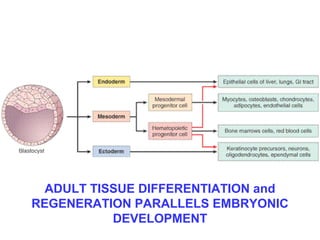





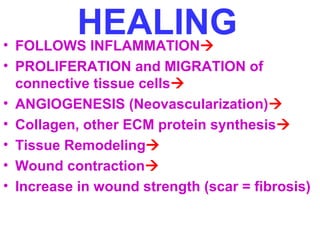
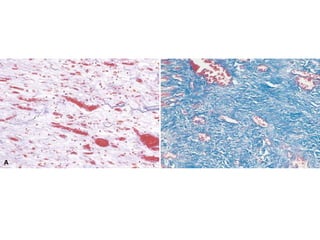
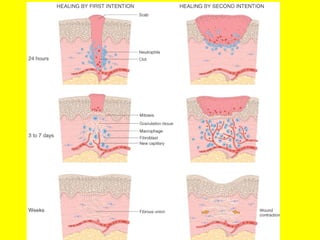
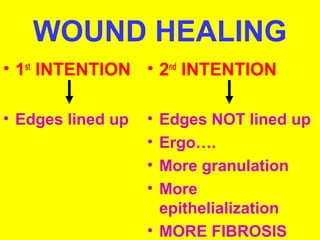
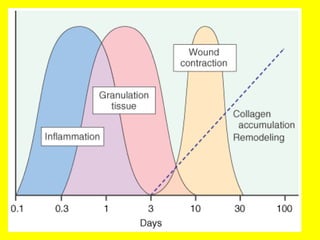



Cell proliferation, growth factors, angiogenesis and the extracellular matrix are key to tissue regeneration and healing. Regeneration replaces lost structures through cell differentiation and proliferation, while healing is the body's response to injury through inflammation, granulation tissue formation, collagen deposition and fibrosis. Many cell types and growth factors interact in healing, with macrophages, platelets and fibroblasts playing important roles in signaling and forming new blood vessels and matrix to repair damage.


















































































