
Downloaded 55 times

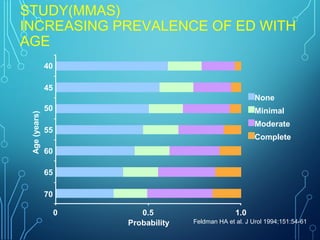
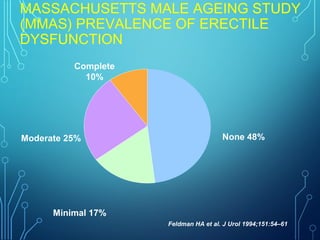
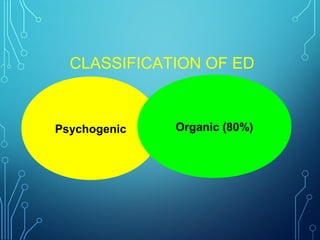
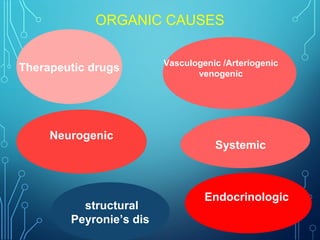
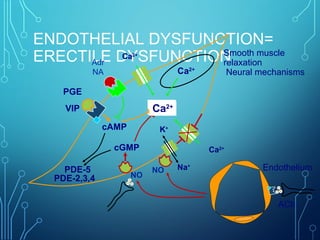
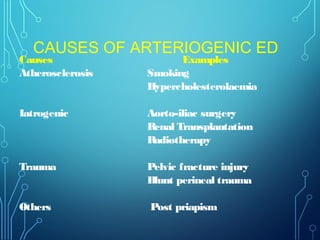
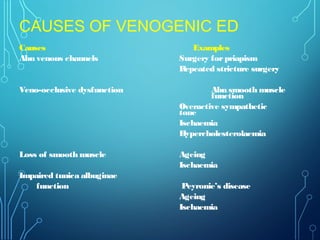
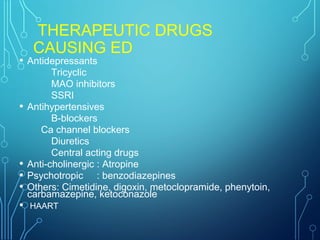


The document discusses the epidemiology, risk factors, pathophysiology, and treatment options for erectile dysfunction (ED), defining it as the inability to achieve or maintain an erection suitable for sexual performance. It highlights various causes of ED, including psychogenic, organic, neurogenic, and hormonal factors, and lists treatment modalities such as lifestyle changes, pharmacological agents, local therapies, and surgical options. The document emphasizes the importance of considering cardiovascular health in patients with ED and the need for a multidisciplinary approach in managing the condition.




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




