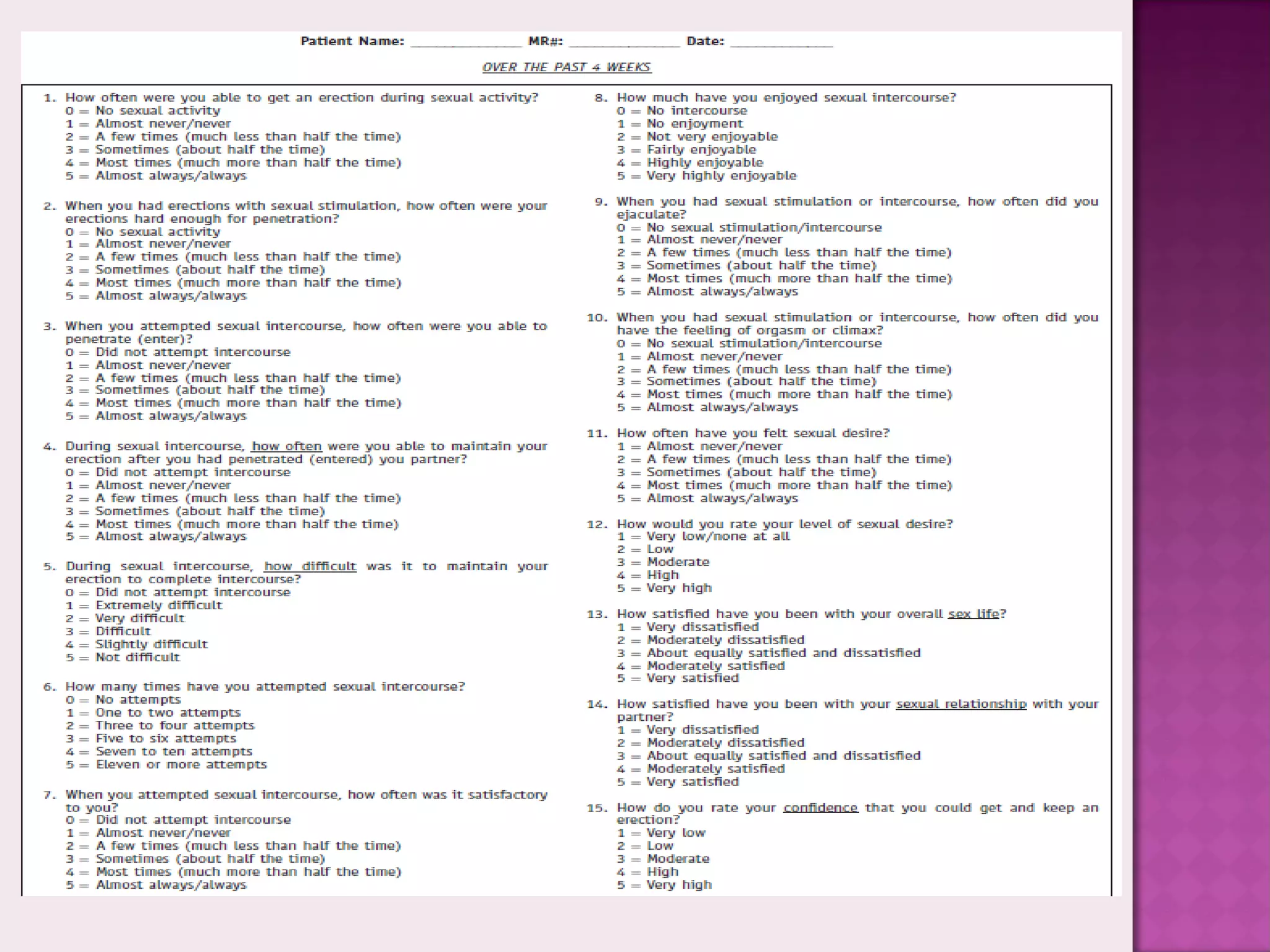
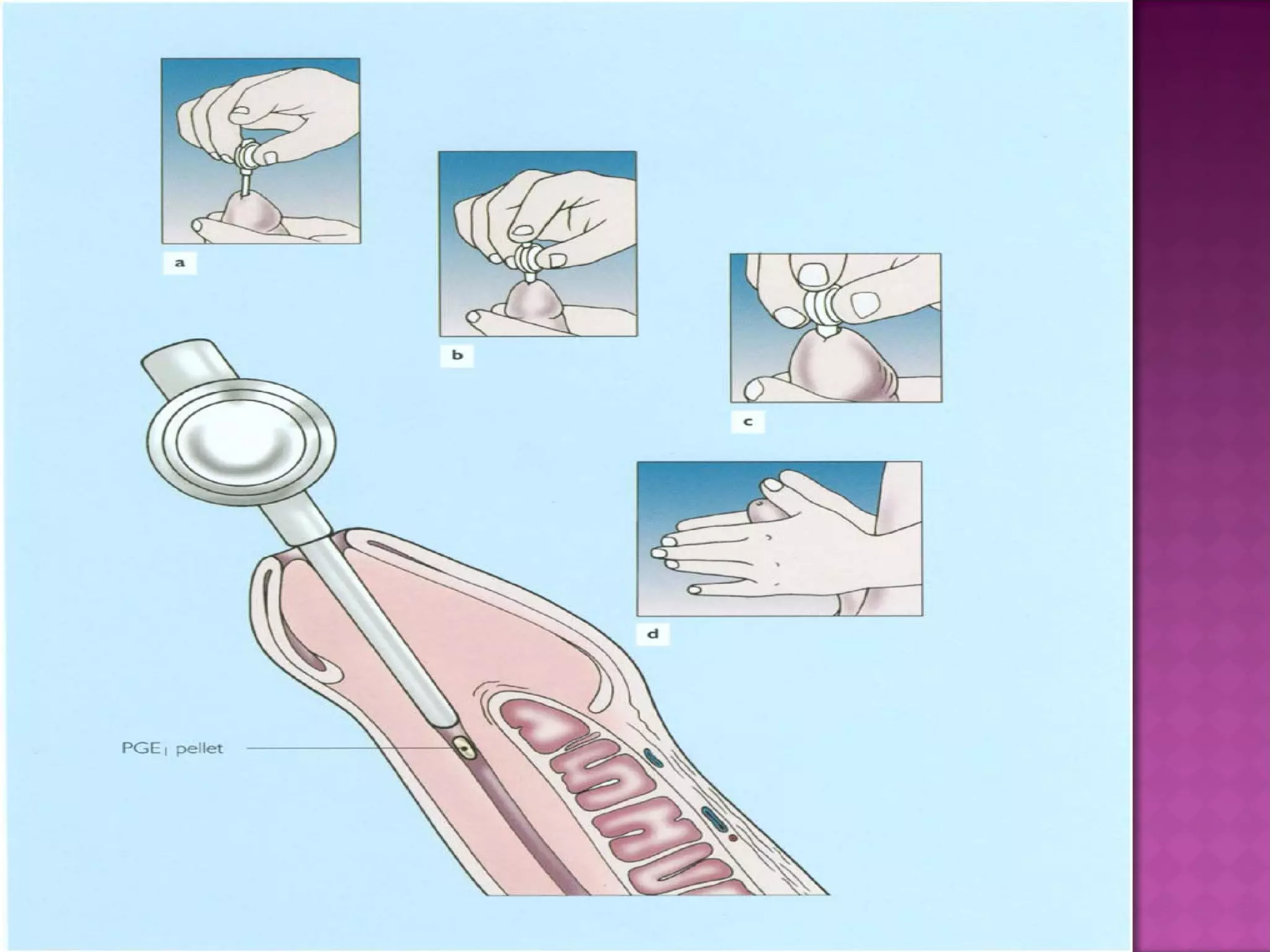
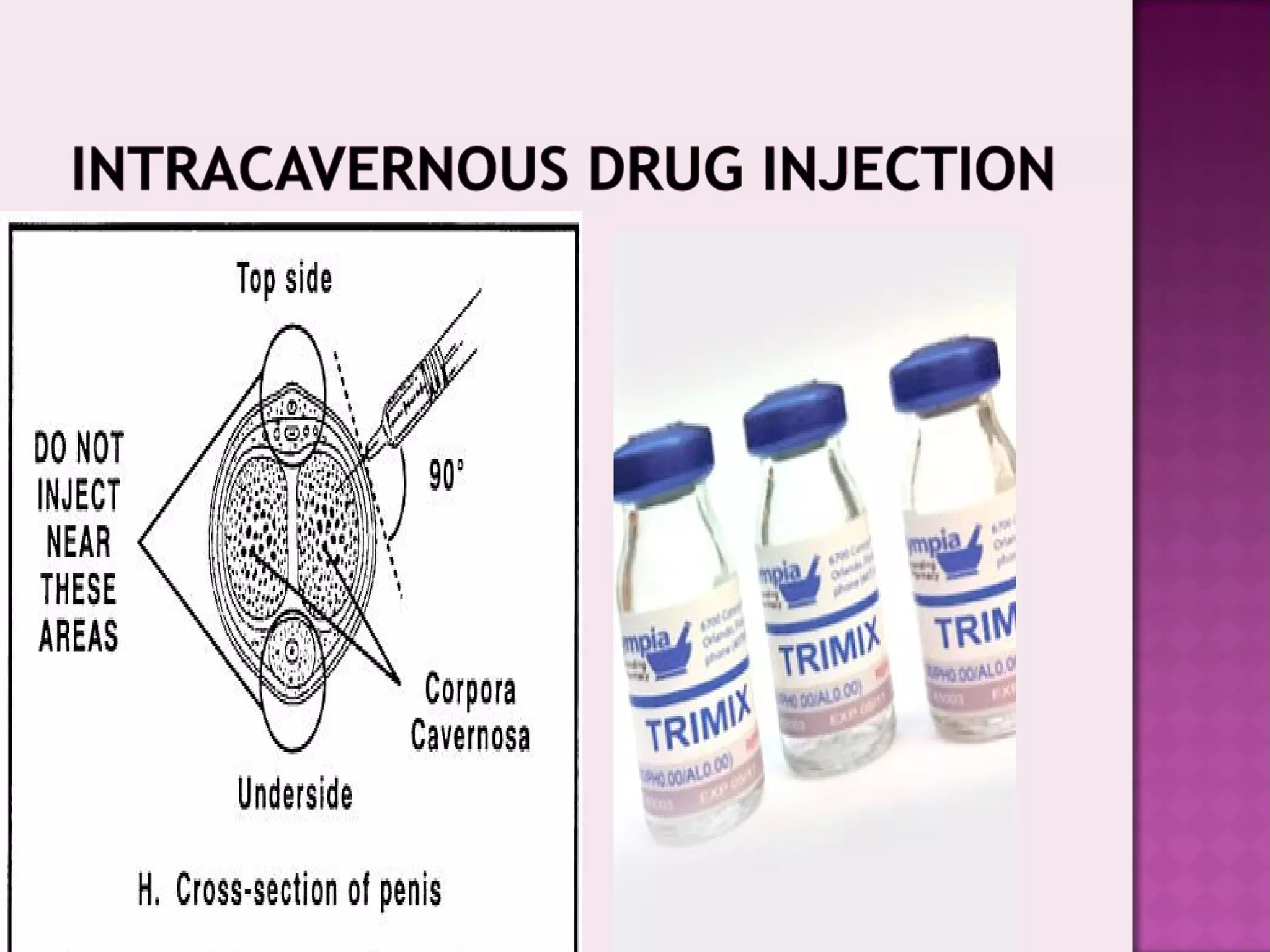
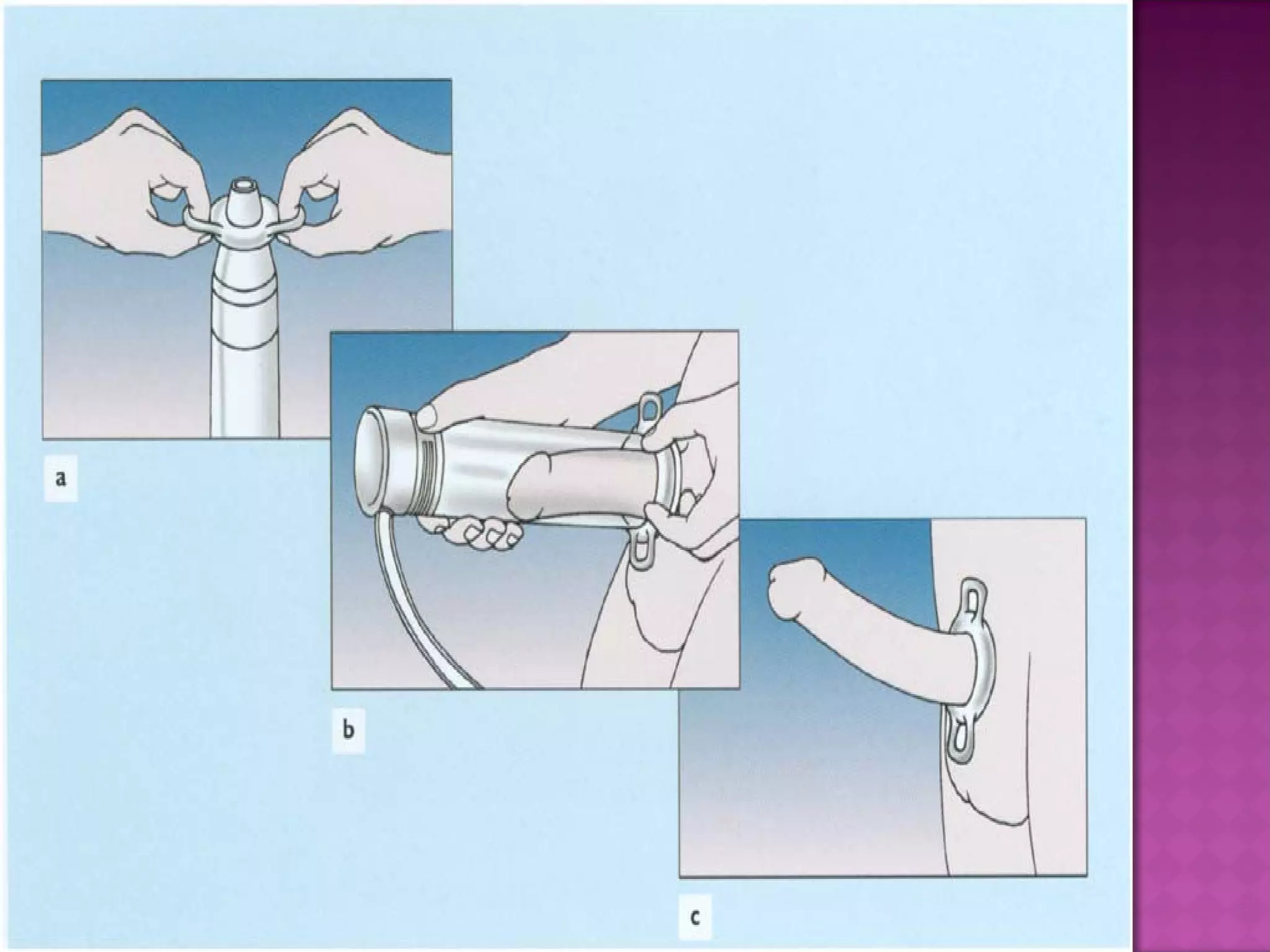
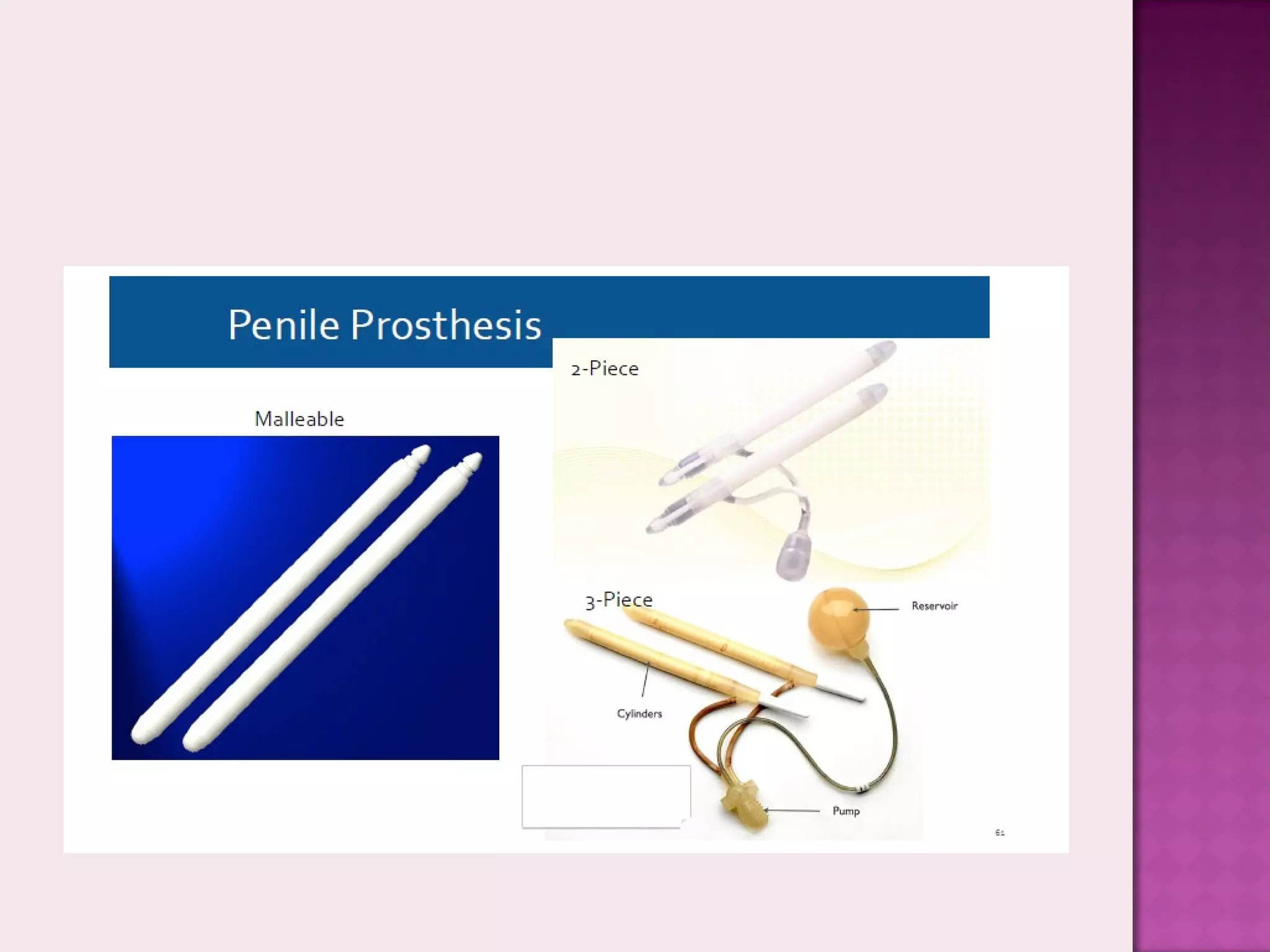
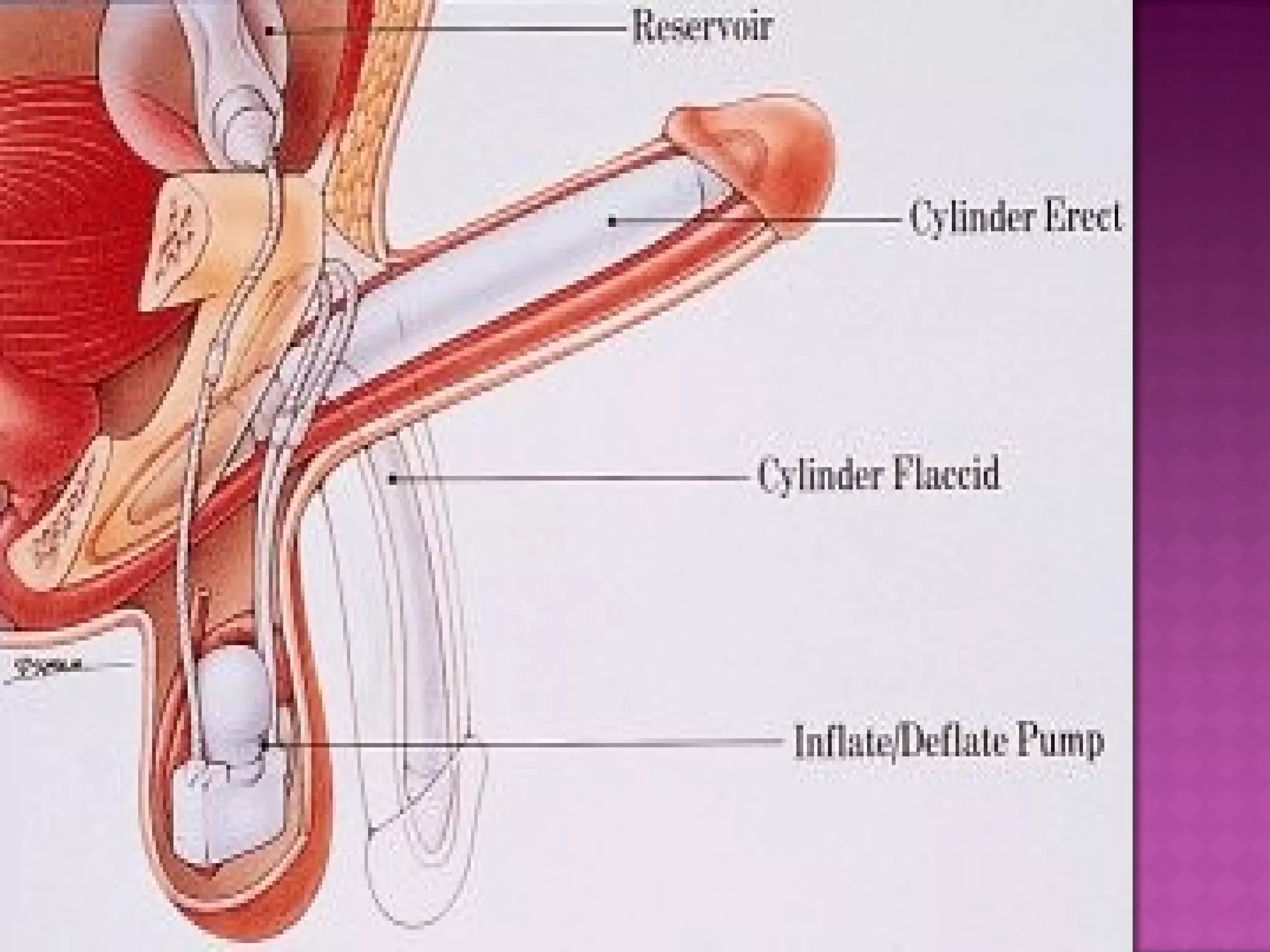
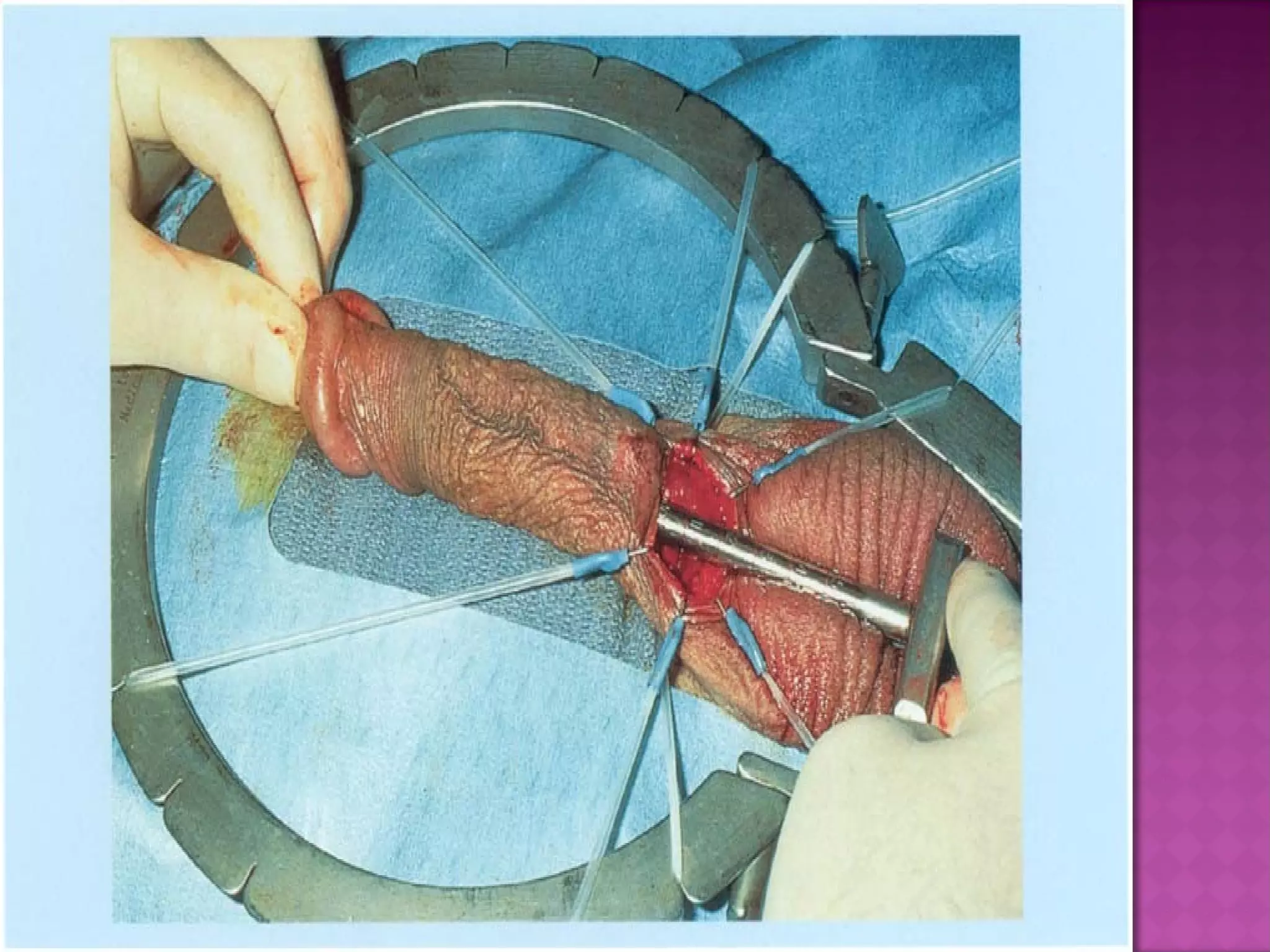
The document discusses the evaluation and treatment of erectile dysfunction. It states that the primary goals in managing ED are to determine the underlying cause, treat reversible factors through lifestyle changes and managing comorbidities, and treat the condition rather than just the symptom. The most common first-line treatment is phosphodiesterase type 5 inhibitors, but other options include penile injections, vacuum devices, and penile prostheses if other treatments fail.









![Erectile Dysfunction [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/ededmond-140716212750-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



























































