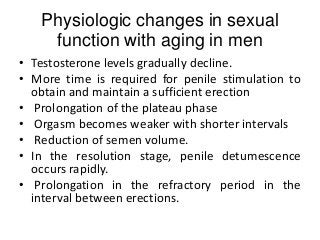
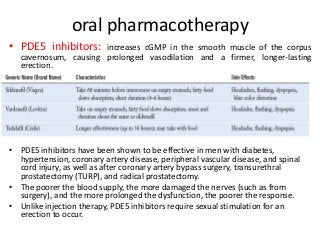
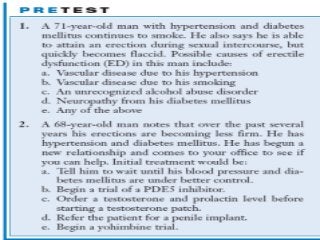
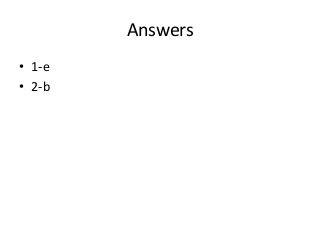

This document discusses erectile dysfunction (ED), including its causes, evaluation, and treatment. Physiologic changes with aging can include declining testosterone and longer refractory periods between erections. ED is defined as the inability to attain or maintain an erection for satisfactory sex. Common causes of ED include vascular diseases, neurological disorders, medications, psychological factors, and endocrine abnormalities. Evaluation involves history, exam, and tests. Treatment options include lifestyle changes, counseling, oral medications like PDE5 inhibitors, penile injections or implants, vacuum devices, and testosterone therapy for hypogonadism.

















































![Erectile Dysfunction [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/ededmond-140716212750-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)