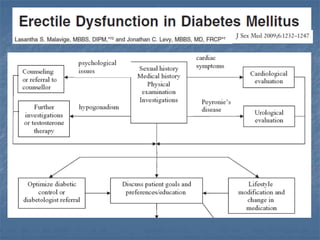
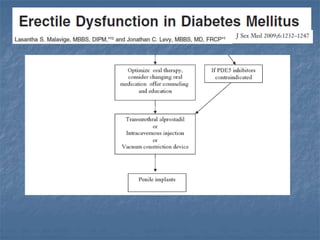
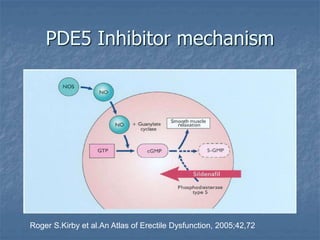
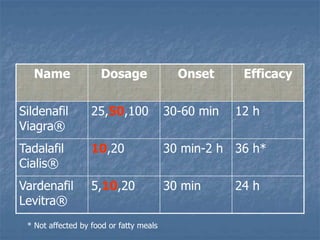
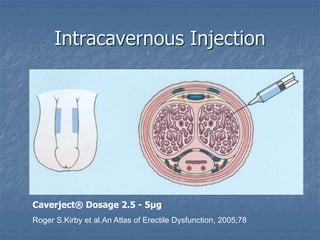
The document discusses the management of erectile dysfunction (ED) in diabetic patients, highlighting that ED is a symptom indicating underlying issues rather than a standalone disease. It outlines diagnostic methods like the International Index of Erectile Function (IIEF-5) and emphasizes the importance of addressing risk factors, controlling blood glucose, and lifestyle changes in management. Treatment options include oral medications, such as PDE5 inhibitors, lifestyle modifications, and surgical interventions like penile prostheses.