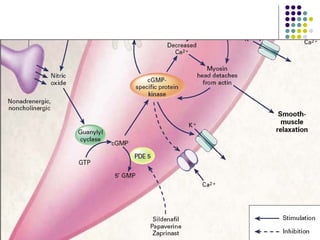
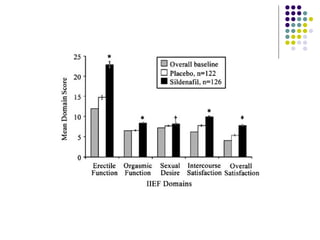
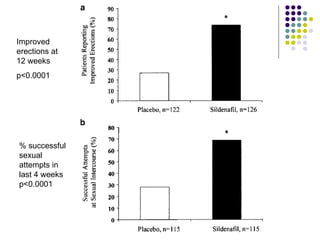
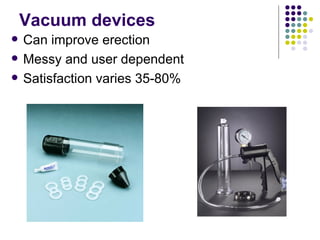
Erectile dysfunction (ED) is common, affecting over 150 million men worldwide. It is a marker for other neurovascular complications in diabetes. The causes of ED include vascular, neurological, endocrine, and psychological factors. Treatments include oral phosphodiesterase type 5 inhibitors, vacuum devices, intracavernosal injections, testosterone replacement, and psychosexual counseling. Managing associated conditions and hormonal deficiencies can effectively treat ED.
















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







