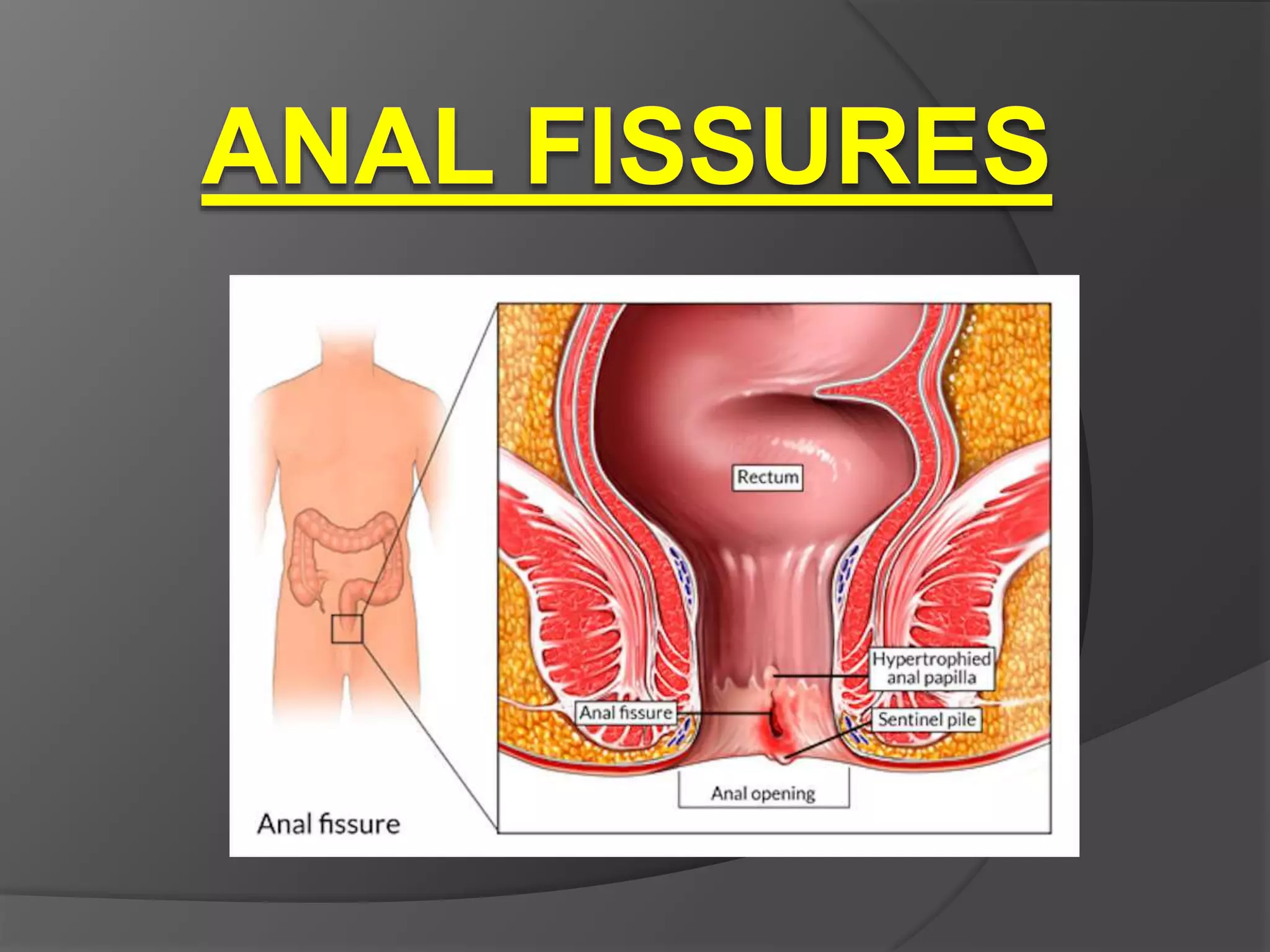
An anal fissure is a small tear in the anal lining that causes severe pain and bleeding during bowel movements. It is often caused by passing hard stool or straining during bowel movements. Symptoms include pain during and after bowel movements, bleeding, and visible cracks. Diagnosis involves visual examination, and treatment focuses on pain relief, increasing blood flow to promote healing, and surgery if it becomes chronic.