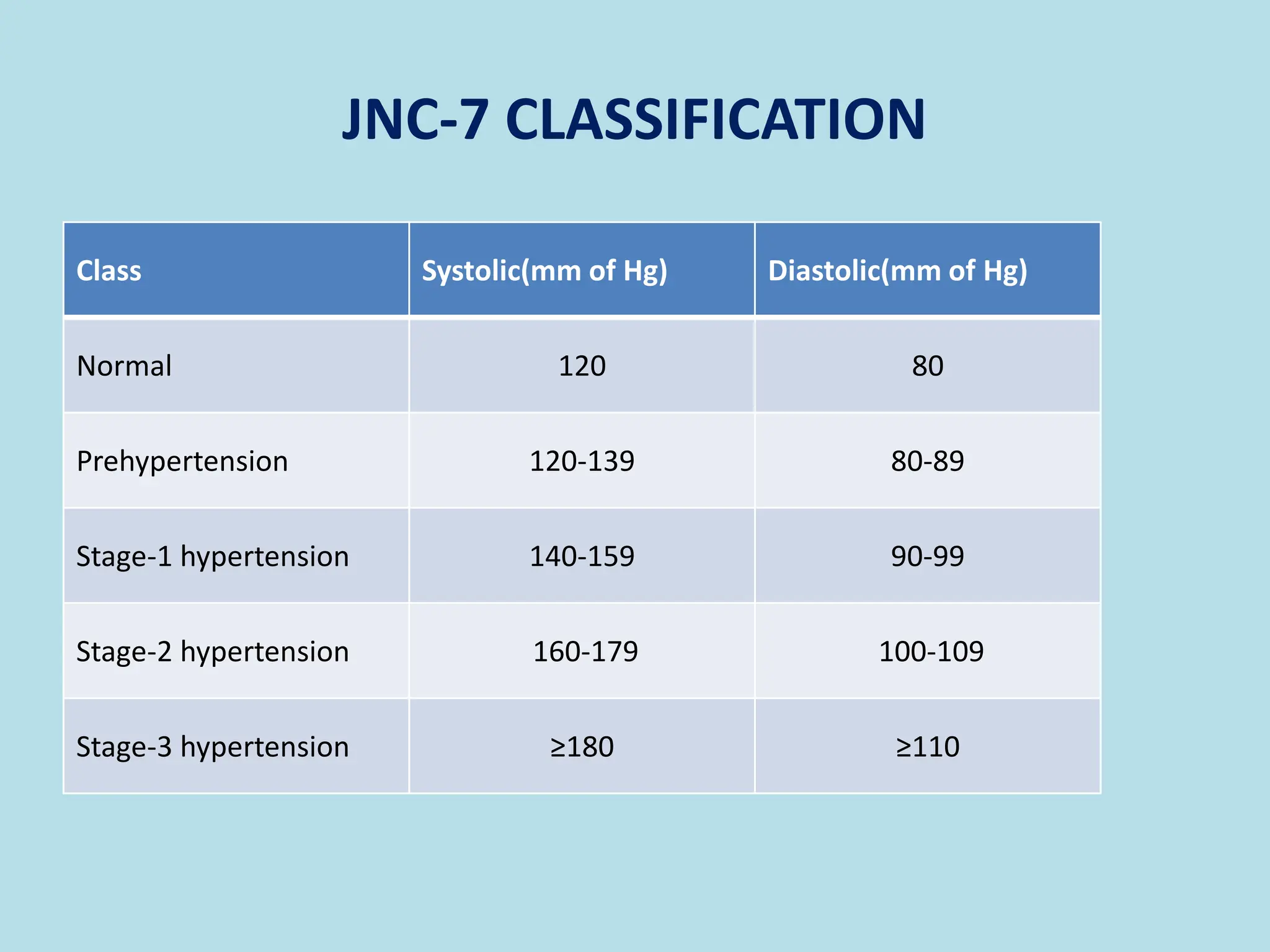
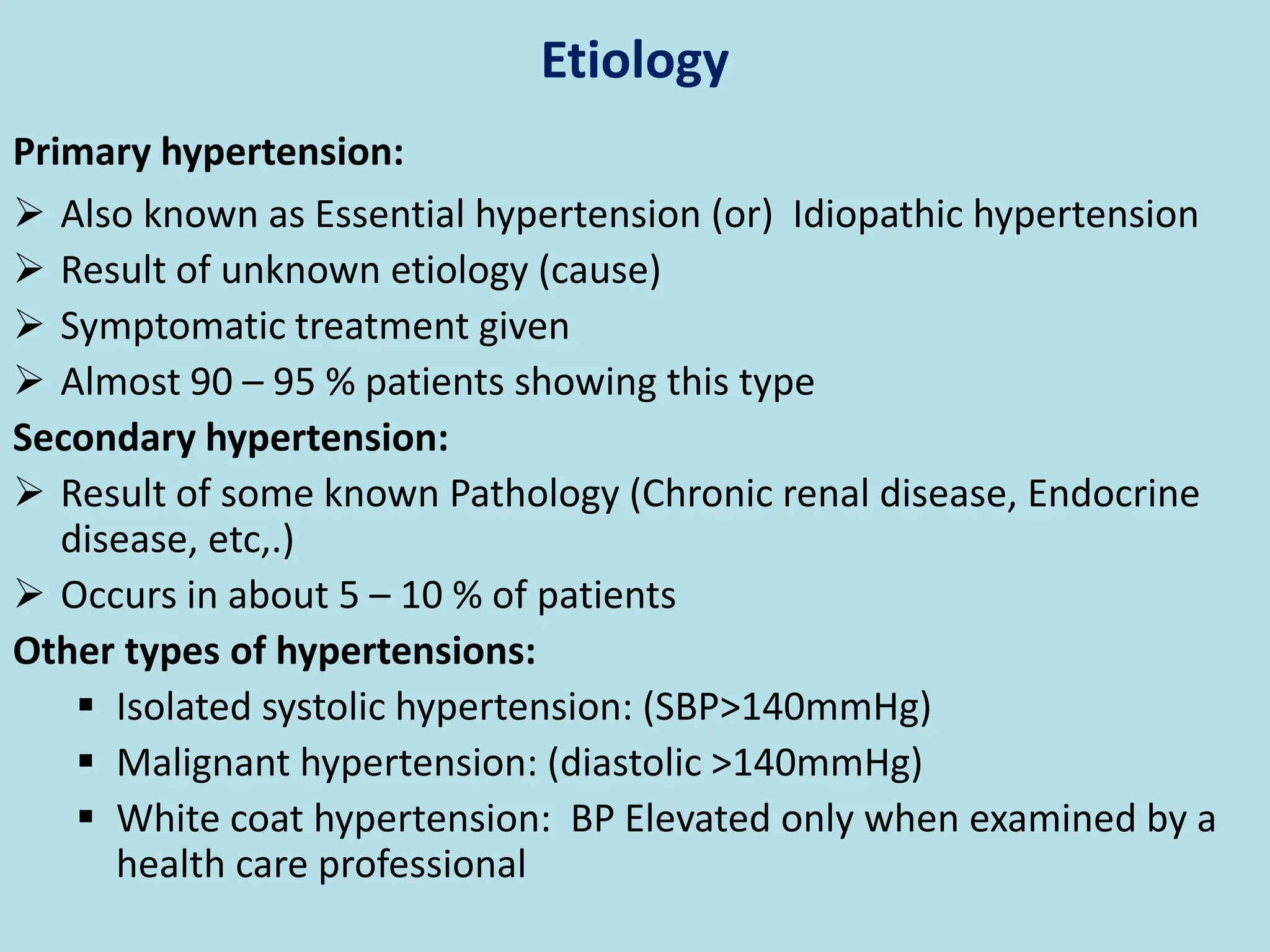
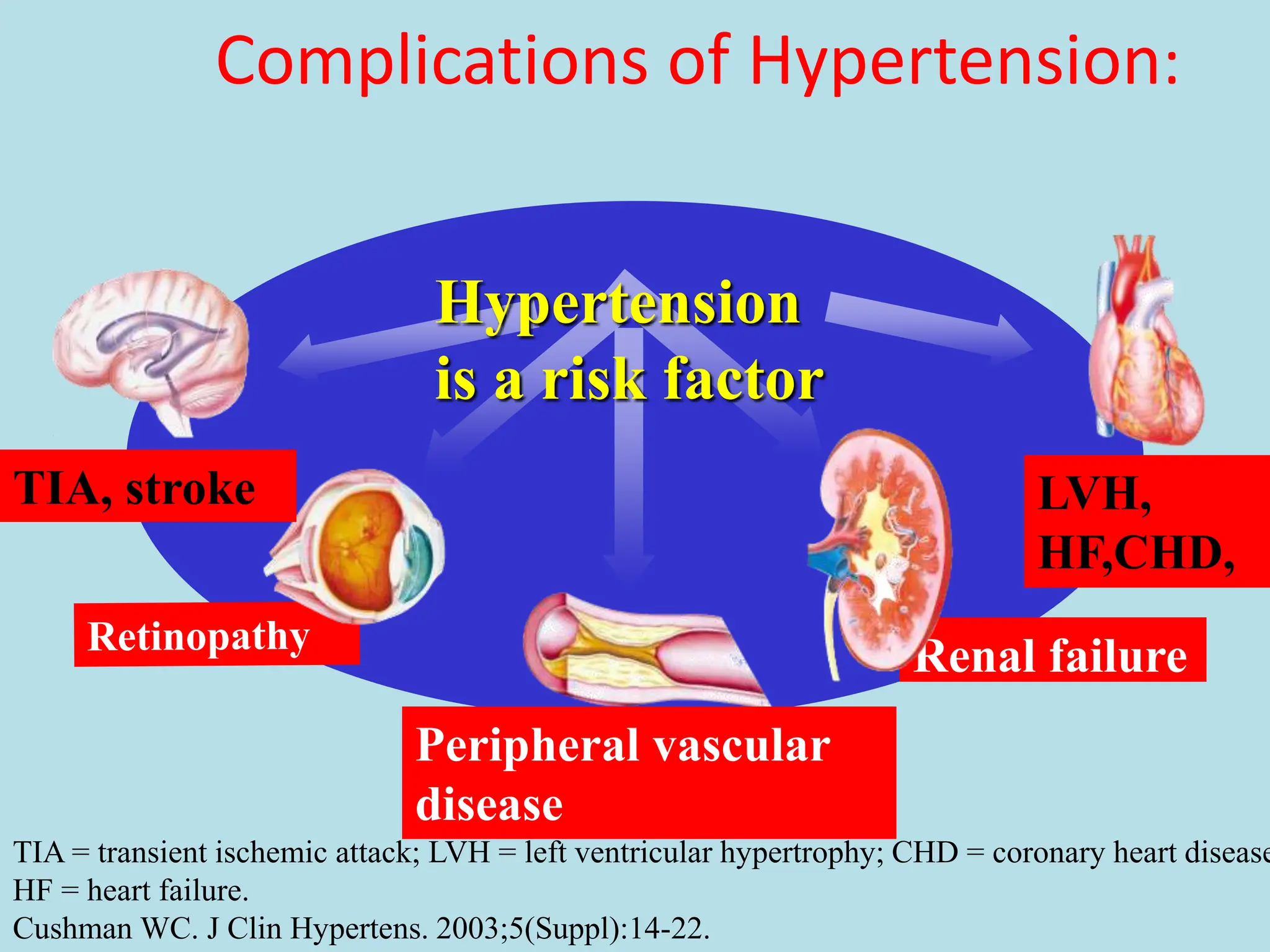
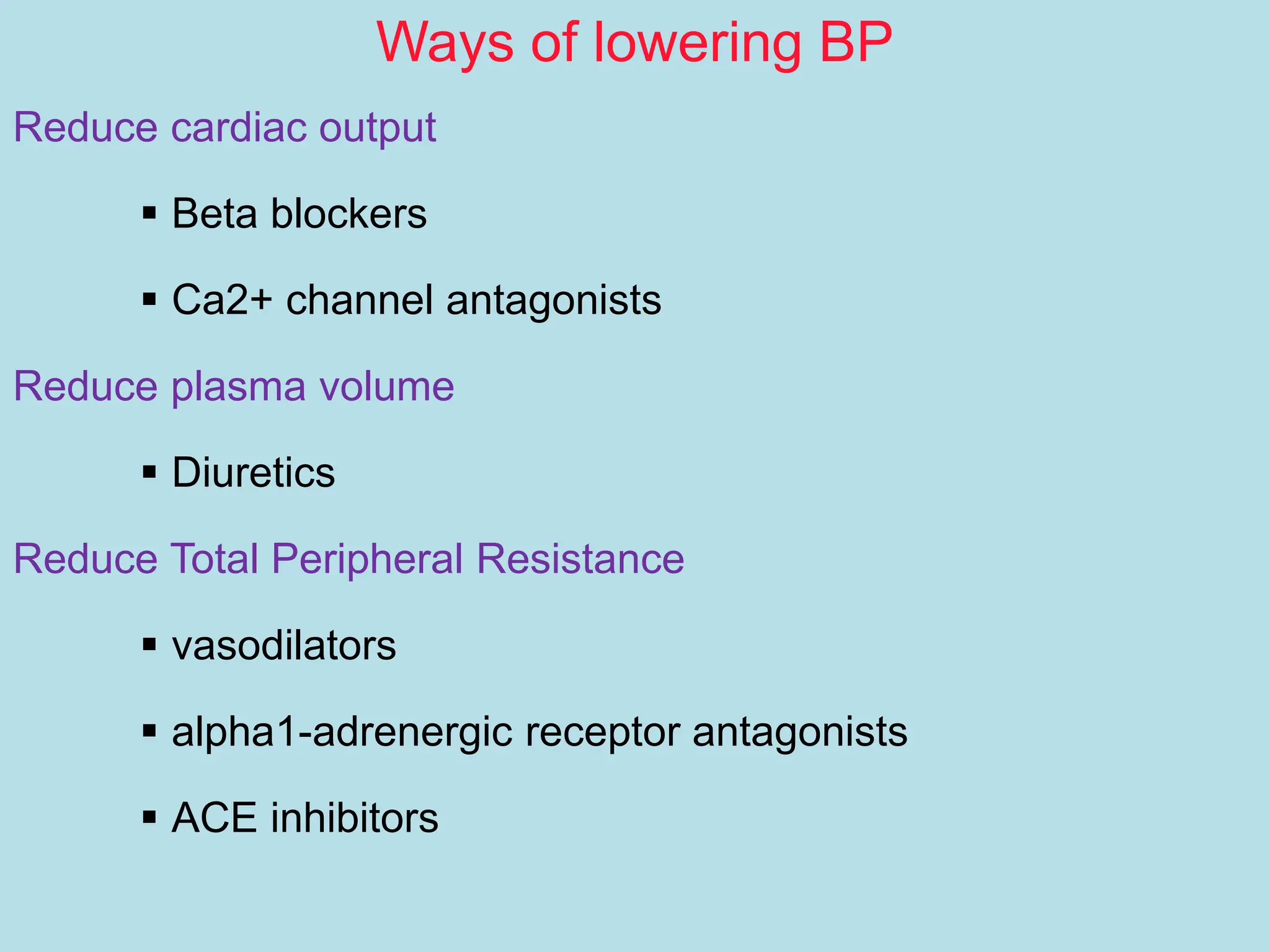
The document discusses hypertension, highlighting its significance as a 'silent killer' with no initial symptoms but severe long-term complications such as heart disease and stroke. It categorizes types of hypertension, factors influencing blood pressure, and emphasizes the importance of public awareness and diagnosis. Management strategies include lifestyle modifications and pharmacological interventions aimed at reducing blood pressure to safe levels.


![Factors Influencing
Blood Pressure (BP)
Cardiac output is total blood flow through systemic or pulmonary
circulation per min. CO =stroke volume (amt pumped out of
L ventricle per beat [70 ml]) times the HR for 1 min.
SVR + force opposing movement of blood in vessels;
determined primarily by radius of small arteries & arterioles
Blood
Pressure
Cardiac
Output
Systemic
Vascular
Resistance
= x
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.](https://image.slidesharecdn.com/hypertension-240109130526-424dc66f/75/hypertension-definition-causes-diagnosis-pptx-3-2048.jpg)