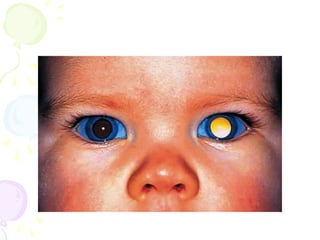
This document provides information on retinoblastoma, a rare eye cancer that affects children. It is the most common primary intraocular tumor in childhood. Key points include that it can be hereditary or sporadic, presents most often as leukocoria, and if left untreated can be fatal. Treatment options described are various localized therapies as well as enucleation if needed. Differential diagnoses discussed include persistent hyperplastic primary vitreous, retinopathy of prematurity, ocular toxocariasis, and Coats' disease.








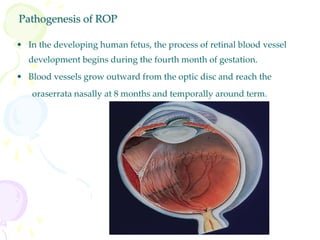
![RETINOPATHY OF PREMATURITY
• bilateral disease and rarely present at birth
• In the 1950s accounted for almost half of causes of blindness in
children in European countries and USA; currently accounts for 10%
blindness.
• Classically, ROP develops in premature infants who have received
supplemental oxygen therapy.
• Infants weighing less than 1500 g at birth and those born at a
gestational age of less than 32 weeks are at risk for developing ROP.
Currently In industrialized countries due to improved monitoring
only neonates with ELBW [ <1000gm]are affected.
• Length of time in oxygen and mechanical ventilation are other risk
factors](https://image.slidesharecdn.com/0001leukocoria-230422115740-11ef4f30/85/0001-leukocoria-ppt-14-320.jpg)