Complications of cataract surgery by Dr. Iddi.pptx
Apply pressure on globe to prevent further drop
Surgeon: Stop phaco, inject OVD, pars plana vitrectomy to remove nucleus
Prevention: Stable AC, well constructed CCC, proper hydrodissection, dispersive OVD
Complications of cataract surgery by Dr. Iddi.pptx
1.
COMPLICATIONS OF
CATARACT SURGERY
PR E S E N T E R : D R . I D D I N D YA B AW E
M O D U L ATO R : D R . L U S O BYA R E B E C C A
M A K E R E R E U N I V E R S I T Y, D E PA R T M E N T O F
O P H T H A L M O LO G Y
M A R C H , 2 0 2 1
2.
OUTLINE
• 6 S’
•Preop complications
• Operative
• Early postop
• Late postop
3.
6 S’
• Selection
•Sterility
• Soft eye
• Safe surgery
• Spectacles
• Sequealae (postop complications)
4.
PREOP COMPLICATIONS
• Anxiety
•Nausea and gastritis
• Irritative or allergic conjunctivitis
• Corneal abrasion
• Complications due to local anaesthesia: Retrobulbar hemorrhage, OCR, Subconj
hemorrhage, spontaneous dislocation of lens into vitreous
5.
RETROBULBAR HEMORRHAGE
• Defn:accum. of blood in retrobulbar space
• C/O: severe pain, loss of vision, N&V.
• O/E: subconj hemorrhage, eyelid ecchymosis, eyelid hematoma, proptosis, elevated
IOP,
• Incidence: 0.1-0.3%
• RFs: preop aspirin, HTN,
• Fear: vascular compromise to optic nerve may result in vision loss!!!
6.
MANAGEMENT
• Inform surgeonimmediately. Intervene in first 2 hours of onset!!!
• Check pulsation of CRA,
• Lateral canthotomy and cantholysis: decompresses the orbit
• Surgical evacuation of infraorbital hematoma if above fails… localized conj peritomy
• Inferior lateral orbitotomy
• Ocassional A/C paracentesis
• Medical mgt:
• I.V Acetazolamide 500mg
• I.V Hydrocortisone 100mg
• Immediate pressure bandage after instilling one drop of 2% Pilocarpine, then postpone op
for 1 week is advised. (IME)
7.
OCR
• Ak.a: Aschnerreflex; trigeminovagal reflex
• RFs: orbital injection, direct pressure on globe, elevated IOP
, paed age
• Cardiac manifestations: bradycardia, ectopic beats, nodal rhythms, AV block, Cardiac
arrest, V fib, V, tach, Asystole
• Caution: EKG monitoring must be performed during all ophthalmic surgeries
• Plan: If mild OCR: resolves alone after removing pressure from globe.
• If severe OCR, I.V Atropine 0.4mg or 0.01mg/kg
8.
INTRAOPERATIVE COMPLICATIONS
• SRlaceration
• Excessive bleeding
• Incision related complications
• Cornea related complications
• Iris related complications
• Capsulotomy related complications
• PCR
• Zonular dehiscence
• Vitreous loss
• Nucleus drop in vitreous
• Posterior loss of lens fragments
• Expulsive choroidal hemorrhage
• IFIS
9.
INCISION RELATED COMPLICATIONS
•Button-holing of anterior wall of tunnel
• Due to superficial dissection of scleral flap
• Plan: use deeper plane from other side of
incision
10.
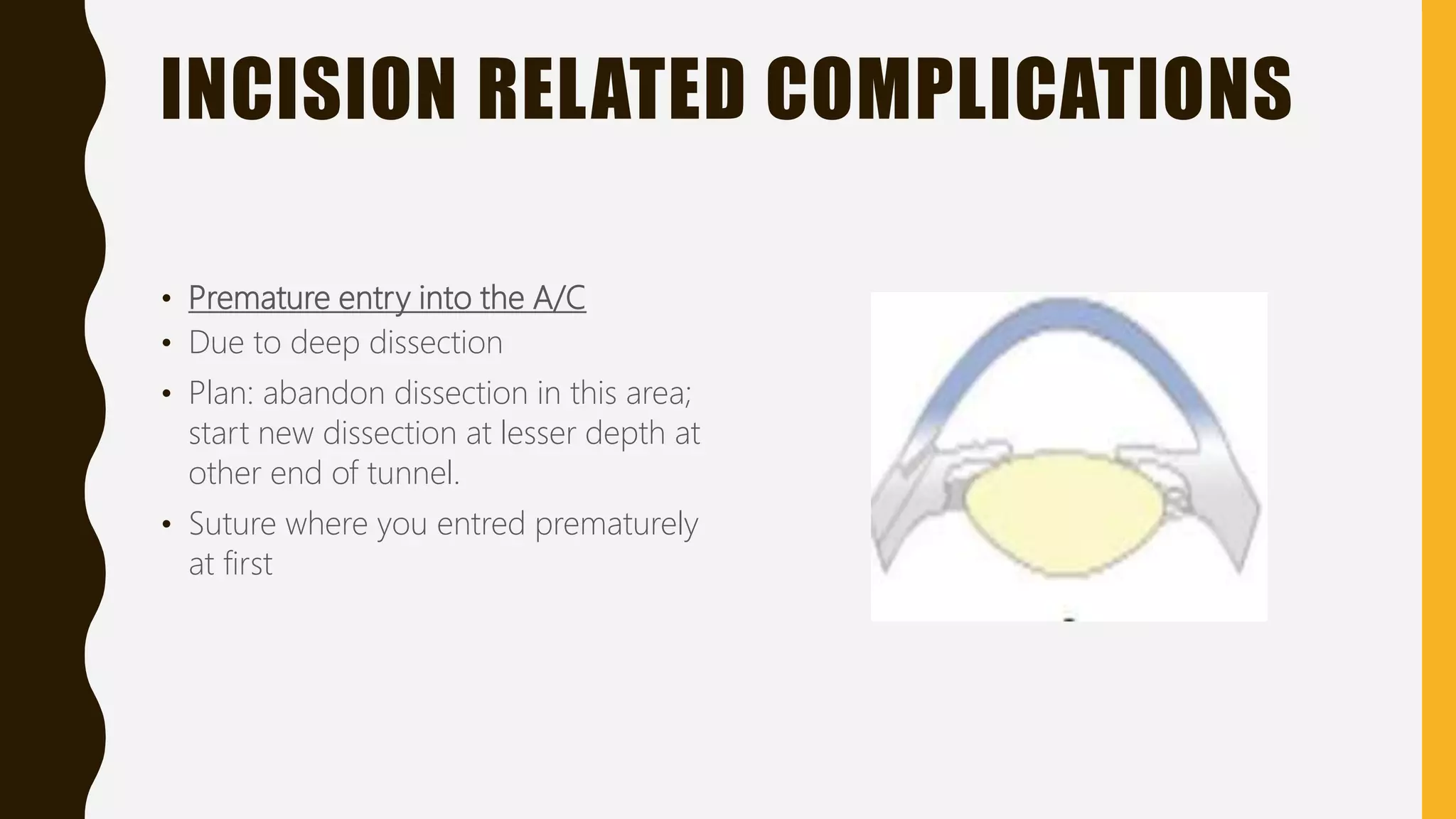
INCISION RELATED COMPLICATIONS
•Premature entry into the A/C
• Due to deep dissection
• Plan: abandon dissection in this area;
start new dissection at lesser depth at
other end of tunnel.
• Suture where you entred prematurely
at first
11.
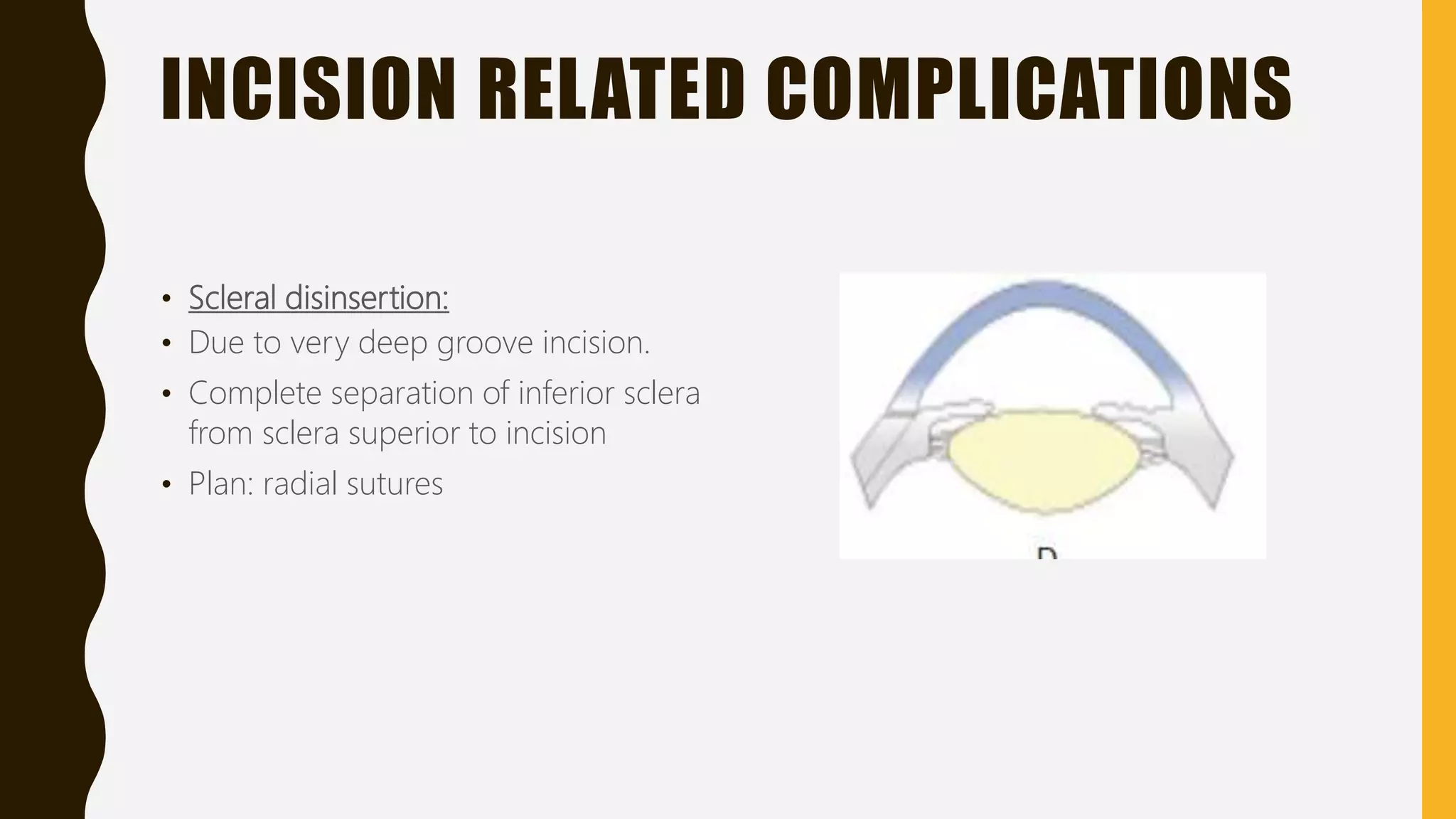
INCISION RELATED COMPLICATIONS
•Scleral disinsertion:
• Due to very deep groove incision.
• Complete separation of inferior sclera
from sclera superior to incision
• Plan: radial sutures
12.
WOUND LEAK
• Increasesrisk of endophthalmitis
• Suture wound if IOP low and/or chamber shallow
• If found post-op with stable AC (no shallowing), stable IOP:
-Aqueous suppressant
-Bandage contact lens
-Follow closely for resolution or need to suture
• Consider wound burn if distorted/difficult to close with suture
• Prevention: Good wound architecture, good surgical technique with instruments in
wound during surgery
13.
WOUND BURN (CONTRACTURE)
•Excess heat released from phaco handpiece can lead to collagen contracture
• Most commonly seen with:
-Inappropriate sizing of wound and tip/sleeve. Can pinch off irrigation (cooling of tip)
Excessive phacoemulsification with full tip occlusion (warning bells signal occlusion)
-Full occlusion eliminates aspiration (key component to irrigation flow)
-Increase phaco power to clear tip, aspirate OVD overlying lens before beginning to
reduce risk of this complication
MGT: suture wound
INJURY TO THECORNEA
• Descement’s membrane detachment (stripping)
• 43%
• Rx: expansile gas (air) tamponade in AC or using SF6, C3F8, suture back large
detachments
GENERAL PRINCIPLE: PROF.BILL
BARLOW
• “The greater the manipulation of the iris, the greater
the miosis, pigment loss, distortion, flaccid nature,
possible bleeding from the minor iris circle or a root
tear”
CYCLODIALYSIS
• Separation ofciliary body from its insertion at scleral spur
• Cause: surgical manipulation of intraocular tissues
• O/E: Gonioscopy shows a deep-angle recess with a gap between the sclera and ciliary
body
• Rx: repair cyclodialysis cleft if hypotony results; closure with argon laser
photocoagulation
COMPLICATIONS RELATED TO
ANTERIORCAPSULORRHEXIS
• CCC is preferred technique in MSICS and phaco.
• Complications:
• Escaping capsulorrhexis: moves peripherally, can even go to posterior capsule. Caused by
shallow AC or poor direction of cystitome. Avoidance: force of cutting cystitome centripetally or circumferencially. Down and
inward force!
• Small capsulorrhexis: predisposes to PCR and nuclear drop during hydrodissection. Rx:
enlarge it by 2-3 relaxing incisions before proceeding further
• Very large capsulorrhexis: difficulty in implanting IOL in bag
• Eccentric capsulorrhexis: can cause IOL decentration
POSTERIOR CAPSULAR RUPTURE
(TEAR)
•Causes:
• -During forceful hydrodissection
• -By direct injury with some instrument e.g Sinskey’s hook, chopper or phacotip
• -During cortex aspiration (accidental PCR)
• -With insertion or rotation of the IOL
• Rate: 2-3%
40.
PCR WITH VITREOUSLOSS
INCREASES RISK FOR:
• Endophthalmitis
• Glaucoma
• Bullous keratopathy
• Suprachoroidal hemorrhage
• CME
• RRD
• IOL malpositioning
• Need for further surgery
• Increased surgical time and cost
41.
MANAGEMENT OF PCR
•Best management is PREVENTION:
• Stabilize the AC by:
-Well-constructed wound and capsulorrhexis
-Proper fluidics setting (Inflow=outflow): helps to avoid post-occlusion surge
• Instruments:
-Dewey phaco tip (rounded vs sharp edge)
-Soft silicone irrigation/aspiration (I/A) tip
• Surgical techniques:
-Protect capsule with second instrument with final fragment (s) emulsification
-Hydrodissection using dispersive viscoelastic (in select cases) or placement of
viscoelastic to tamponade capsule
42.
PCR: PREVENTION
• Recognisinghigher risk surgical situations:
• Weakened posterior capsule; posterior polar cataract
• Dense (white or brunescent) cataract: little to no cortex to ‘mold’ capsule
• Soft nucleus (e.g young patient with PSC): not much energy needed to penetrate
material
• Zonular weakness:
-PXF,
-prior trauma,
-prior intraocular sugery (e,g PPV)
-Less common causes: congenital; aniridia etc
43.
RISK FACTORS FORPCR
• OCULAR FACTORS:
• Difficult cataracts (brunescent, morgagnian, PXF, PPC)
• Pre-existing zonulysis/subluxated cataracts
• Glaucoma
• High myopia
• Increase in vitreous pressure observed after retrobulbar anaesthesia
• Small pupils
• Poor visibility (corneal opacities – scar, shagreen, arcus, band K, pterygium, poor
surface)
44.
OTHER RISK FACTORSFOR OCR
• PATIENT FACTORS:
• Hypertension
• Chronic lung disease
• Obese patient with short thick neck
• Uncooperative
• Demented
• High nose bridge
• Deep seated eyes
• INTRAOPERATIVE FACTORS:
• Small CCC
• Unstable AC
• Wound distortion – striae
• Inappropriate phaco settings
• Zonulysis
• OTHER FACTORS:
• Inexperienced surgeon
• Poor operating microscope
• Inadequate sedation/anaesthesia
45.
CLINICAL SIGNS OFPCR
• Presence of ring reflex in the posterior capsule – outline of PCR seen
• Inability to aspirate soft lens matter (vitreous stuck to port)
• Poor followability of nuclear fragments, inability to rotate a previously mobile nucleus
• Peaked pupil
• Vitreous seen in AC
• Sudden deepening of AC and PC
• Fragments disappear from view
• Pupil-snap sign: PC rupture during hydrodissection
• Movement of iris with phaco probe due to vitreous strands
46.
PCR MANAGEMENT GOALS
•Every maneuver is made to avoid extending tear
• Maintain chamber stability: pressure gradient drives vitreous
• No irrigation toward tear/vitreous: hydration of vitreous/disruption of vitreous
• Use OVD copiously but not excessively: fill space with OVD to control gradient; overfill can propagate tear
47.
PCR MANAGEMENT DEPENDSON:
• Stage of operation at which PCR occurs, commonly during:
-Nucleus expression/removal of last fragment
-Aspiration of soft lens
-IOL insertion
• Size and extent of PCR
• Presence or absence of vitreous loss
MANAGEMENT OF PCR
•Stop the surgery and assess the situation
• Evaluate location and size of tear; this will determine response.
• Don’t suddenly remove instruments as it would decompress the AC, causing extension of
the capsular tear and further enabling the vitreous to prolapse forward.
• Instead, maintain the phaco needle’s position and continue to irrigate without aspiration.
• Next, inject a dispersive viscoelastic through the side port in the area of capsular
compromise.
• In addition to stabilizing the anterior chamber, this helps to push back any vitreous and
maintains the integrity of the anterior hyaloid face.
• Only now can the phaco tip be removed from the eye.
NO VITREOUS LOSS!MGT OF NUCLEUS
• Avoid loss of nuclear material through PCR into posterior segment.
• Removal of nucleus should be done carefully, using either a dispersive viscoelastic bed or a
surgical glide for protection.
• If there are large fragments of nucleus remaining, they should be phacoemulsified in the
anterior chamber. Use dispersive viscoelastic to maintain the chamber and keep vitreous
away from the phaco needle.
• If most of the nucleus remains, and PCR is large, convert to ECCE, remove nucleus with lens
loop or spoon.
• Not recommended to retrieve nuclear fragments from deep vitreous. If in anterior vitreous,
do anterior vitrectomy, remove cortex and place sulcus IOL, but leave nucleus removal to a
VR colleague
52.
IF THERE ISVITREOUS LOSS!!!
• If vitreous prolapse has occurred, remove all vitreous from A/C
• Vitrectomy reduces chance of vitreoretinal traction or vitreous adherence to IOL.
• Vitreous may be stained with unpreserved triamcinolone for better visualization. Avoid
manually externalizing and cutting the vitreous through the incision… RD
• Options: 2-port anterior vitrectomy, PPV
• Vitrectomy settings:
-Cut I/A mode
-High cut rate
-Low aspiration rate
-Separate irrigation
-Consider Pars plana approach for vitrector (select cases)
53.
IOL PLACEMENT
• Stabilityof remaining capsule!
• If posterior capsule support for intracapsular placement of IOL is inadequate, preserve
the anterior capsule to enable capture of lens optic in capsular bag with haptics placed
in ciliary sulcus. 3-piece IOL with TD of 12.5mm
• A single piece acrylic IOL is not suitable for the ciliary sulcus because of possibility of
UGH, decentration
• With absence of capsular support :
-A PC IOL can be used, suturing the haptics to the iris or by fixing haptics to the sclera
through the ciliary sulcus. (reduce power by 0.5D)… Osher Bounce test
-Insert AC IOL, particularly in elderly patients. Add 1mm to HCD.
-Leave aphakic (large PCR with inadequate posterior capsule support and AC IOL
contraindicated)
Avoid silicone lenses in PCR, higher rates of endophthalmitis
54.
CHECKLIST AT ENDOF OPERATION
• Obvious vitreous at pupil borders?
• Inject miotic agent… round pupil observed?
• Traction at wound edge with weck sponge….. Peaking of pupil? Or movement of iris
when sweeping AC with Sinski (Marionette sign)
• Inject air bubble …. Regular round bubble observed?
• Sweep iris…. Movement of AC?
• Close wound with 10-0 nylon
55.
POST-OP VITREOUS LOSSAFTER PCR
• If vitrectomy was required, a thorough dilated exam in the early post-op period is
indicated to evaluate for retinal pathology
• Post-op presentation of vitreous:
• If vitreous is entrapped in wound, risk of ‘wicking’ present, infection risk elevated.
-can stain at slit lamp with fluorescein (bright green temporary stain) if externalised. Take
to OR for removal is this is the case
-If vitreous is incarcerated in wound, but not externalised, can consider YG vitreolysis
• Regardless of presentation, must be dealt eith to eliminate traction which creates risk
of retinal tear and CME.
56.
ZONULAR DEHISCENCE
• Ruptureof the fibrous strands connecting the ciliary body and the crystalline lens of
the eye
• RFs:
-PXF
-Extraocular trauma
-Surgical trauma
-Marfan’s syndrome
-If patient had RD, and silicone oil used to fix the detachment
O/E: lens jiggles when patient to look back and forth
Rx: CTR. Cionni type 1L for right handed, and 2C for left handed.
VITREOUS LOSS
• Mostfeared complication after PCR.
• Prevention:
• To decrease vitreous volume;
-preop use of hyperosmotic agents like 20% mannitol or oral glycerol
-to decrease aqueous volume: preop: Acetazolamide 500mg orally
-to decrease orbital volume: adequate ocular massage and orbital compression using:
superpinky, Honan Ball, or 30mmHg of Paed sphygmomanometer
• If vitreous loss has occurred; aim is to clear it from the AC and incision site. Anterior
vitrectomy
NUCLEUS DROP INVITREOUS CAVITY
• More common in phaco; high pressure AC system; less in MSICS
• TYPES:
-prior to nucleus removal
-during nucleus removal
-after nucleus removal
Signs of impending nucleus drop:
-runaway capsulorrhexis
-pupil-snap sign (pupils suddenly constricts)
-nuclear tilt
-receding nucleus
-difficult to rotate nucleus
61.
NUCLEAR DROP
• PREVENTION
•Good sized and shaped
• Careful hydrodissection
• Clear endpoints in nuclear
management
• Recognition of occult PCR
• MANAGEMENT:
• No attempt should be made to
fishout nucleus from the vitreous
• Refer to VR surgeon after a thorough
anterior vitrectomy and cortical
cleanup
POSTERIOR LOSS OFLENS
FRAGMENTS
• After PCR, or zonular dehiscence
• Complications: glaucoma, chronic uveitis, chronic CME, RD
MGT:
• Refer to VR Surgeon; for PPV, and removal of lens fragments
EXPULSIVE CHOROIDAL HEMORRHAGE
•One of most dramatic and serious complications of cataract surgery
• Characterised by spontenous gapping of wound, then expulsion of lens, vitreous,
retina, uvea and finally a gush of bright red blood…. “self-evisceration”!!!
RFs:
• -conventional ECCE
• -ICCE
• -HTN
• -Artherosclerosis
• -chronic lung disease
• -short thick neck (obesity)
• -severe myopia
• -PCR during surgery
• -glaucoma
67.
.• O/E:
• Darkening(loss) of red reflex
• Incision gape
• Iris prolapse
• Expulsion of lens, vitreous, and bright red bloos
• Elevated IOP
• MGT:
• Stop surgery
• Immediate wound closure with 4.0 silk suture
• I.V Mannitol
• Attempt to drain suprachoroidal blood by doing an equatorial sclerotomy (decompresses
the globe)
• Most of the time, eye is lost, so evisceration is done!!!
INTERVENTIONS TO REDUCEEFFECTS
OF IFIS
• Use preoperative atropine
• Intracameral injection of alpha-adrenergic agonists like phenylephrine or epinephrine
• Careful attention to incision location and construction to reduce wound leak
• Use iris hooks or pupil expansion rings for stabilization
• Use of bimanual microincision surgical techniques
• Employment of highly retentive OVDs to ‘viscodilate’ the pupil and maintain a concave
iris near the incision
• Discontinuation of fluid inflow prior to withdrawal of instruments to prevent and iris
egress
• Use of low-flow settings to minimize anterior chamber turbulence and eliminate a
higher pressure gradient posterior to iris
HYPHEMA
• RFs: PXF,Fuch’s heterochromic uveitis, anterior segment neovascularization, vascular tufts at
pupillary margin
• Grades: …Micro, Grade 1, 2 3, 4
• Treatment:
• Most resolve spontaneously
• Resolution might take longer if vitreous is mixed with blood
• If hyphema is large and associated with high IOP
, lower the IOP with acetazolamide and
mannitol.
• If blood isn’t absorbed within one week, then a paracentesis should be done to drain the
blood
• Two major complications: Elevated IOP
, corneal blood staining
• If hyphema occurs several years after surgery, it’s due to incision vascularization,,, do argon
IRIS PROLAPSE
• Risk:inadequate suturing of incision after ICCE and conventional ECCE
• Less with phaco and MSICS
• Plan:
• -A small prolapse of less than 24 hours duration may be reposited back and wound
sutured.
• -A large prolapse of long duration needs abscission and suturing of wound
•
STRIATE KERATOPATHY
• Mildcorneal edema with Descemet’s folds
• Due to endothelial damage during surgery
• Plan: mild striate kertopathy usually disappears spontaneously within one week
• Moderate-severe keratopathy is treated by instilling hypertonic saline drops (5% NaCl)
along with steroids
FLAT (SHALLOW ORNONFORMED)
ANTERIOR CHAMBER
• Due to wound leak, ciliochoroidal detachment or pupil block
• 1) flat AC with wound leak:
-associated with hypotony
-dx: siedel’s test. Fluorescein will be diluted at site of leakage by aqueous
-Rx: pressure bandage for 4 days and oral acetazolamide
If condition persists, injection of air in AC and resuturing of the leaking wound.
2) CILIOCHOROIDAL DETACHMENT
•It may or may not be associated with wound leak
• Presents as a convex brownish mass in involved quadrant with shallow AC
• Rx: pressure bandage for 4 dyas plus oral acetazolamide
• If condition persists , suprachoroidal drainage with injection of air in AC is indicated.
3) PUPIL BLOCK
•Due to vitreous bulge
• After ICCE
• Leads to formation of iris bombe and shallowing of AC
• If condition persists for 5-7 days, permanent peripheral anterior synechiae (PAS) may
be formed leading to secondary angle closure glaucoma
• Pupil block glaucoma is managed initially with mydriatic, hyperosmotic agents (e.g
20% mannitol) and acetazolamide
• If not relieved, then laser or surgical peripheral iridotomy should be done to bypass
the pupillary block
POSTOPERATIVE ANTERIOR UVEITIS
•Can be induced by:
• -instrumental trauma
• -undue handling of uveal tissue
• Reaction to residual cortex or chemical reaction induced by OVDs, pilocarpine etc.
• Mgt:
• -more aggressive use of topical steroids, cycloplegics and NSAIDs
• -rarely systemic steroids may be required in cases with severe fibrinous reaction
89.
TOXIC ANTERIOR SEGMENTSYNDROME
• Defn: an acute sterile postoperative inflammation
• S&S:
• -mimics endophthalmitis
• -photophobia
• -severe reduction in VA
• -corneal edema
• -marked AC reaction
• -occasionally sterile hypopyon
90.
DISTINGUISHING FEATURES OFTASS
• Diffuse limbus-to-limbus corneal edema
• AC fibrinous exudate
• A dilated, irregular or non-reactive pupil
• Elevated IOP
• Pathology limited to AC
• TASS presents within hours of surgery, whereas acute infectious endophthalmitis
develops 2-7 days postoperatively
• Pain in TASS is less than in infection
• PATHOPHYSIOLOGY
• The acute inflammatory response induces cellular necrosis and/or apoptosis as well as
extracellular damage.
RISK FACTORS OFTASS
• Any medication injected in or around the eye or placed topically at the time of surgery
can be implicated in TASS.
• Preservatives and pH incompatibilities can lead to TASS as can contaminants from
sterilization.
• Intraocular solutions with inappropriate chemical composition, concentration, pH, or
osmolality
• - Preservatives
• - Denatured ophthalmic viscosurgical devices
• - Enzymatic detergents
• - Bacterial endotoxin
• - Oxidized metal deposits and residues
• - Intraocular lens residues
93.
PREVENTION AND TREATMENTOF
TASS
• Prevention:
• -careful cleaning, rinsing and air drying
of reusable cannulas
• -using disposable instrumentation
• -avoiding intraocular use of any
nonphysiologic or preserved solutions
• Treatment of TASS:
• -topical steroids
• -systemic steroids
• Frequent follow-up; monitor IOP,
assess for signs of bacterial infection
BACTERIAL ENDOPHTHALMITIS
• Defn:suppurative inflammation of the inner structures of the eyeball
• RFs:
• -DM
• -Older age
• -Male gender
• -Vitreous loss
• -PCR
• -Wound leaks
• -Use of clear corneal incisions
• -Complicated or prolonged surgery
• Can be: acute form or indolent/chronic
96.
S&S OF ENDOPHTHALMITIS
•Symptoms
• -mild to severe ocular pain
• -vision loss
• -floaters
• -photophobia
• Signs
• -vitreous inflammation
• Eyelid or periorbital edema
• Ciliary injection
• Chemosis
• AC inflammation
• Hypopyon
• Decreased VA
• Corneal edema
• Retinal hemorrhages
PREVENTION AND TREATMENTOF
ENDOPHTHALMITIS
• Prevention
• Preop topical antibiotics
• Povidone iodine, 10% and 5%
• Ix: VA, AC tap, Vitreous tap, culture
and gram stain
• Treatment
• Do VA as soon as you suspect
Endophthalmitis
• Blind: evisceration
• Vision better than PL; PPV +
intravitreal antibiotics (vanco) +
topical antibiotics
• If VA is HM and better; do AC tap for
cultures with subsequent intravitreal
injection of antibiotics
100.
.
• Vancomycin 1mg/0.1ml;3 doses on alternate days or
• Ceftazidinme 2.25mg/0.1ml or
• Amikacin 0.4mg/0.1ml
• EVS: Vanco + amikacin
• If improvement seen then, topical and subconj antibiotics
• Chronic or delayed-onset endophthalmitis best treated with vitreous biopsy and
intraocular antibiotics
CME
• A.k.a :Irvine-Gass syndrome
• Common cause of postop decreased vision
• Pathogenesis unknown
• Defn: collection of fluid in the form of cystic loculi in the Henle’s layer of the macula
• Pathophysiology:
• -increased perifoveal capillary permeability with accumulation of fluid in the inner
nuclear and outer plexiform layers
• -associated with intraocular inflammation
• -mediated thru release of prostaglandins and leukotrienes
SURGICAL AND POSTOP RISK
FACTORS
• Posterior capsular rupture
• Vitreous loss
• Iris prolapse
• Prolonged surgical time
• Improper IOL positioning
• Retained lens material/fragments
• Poorly controlled postop inflammation
• Transient or prolonged hypotony
110.
MEDICAL TREATMENT OFCME
• Topical steroids +/- NSAIDS 3/12
• If topicals fail, then subtenon’s steroid injections or intravitreal injections
• In refractory cases, systemic carbonic anhydrase inhibitors may be beneficial
• Intravitreal anti-VEGF in cases not responding to conventional treatment
111.
SURGICAL THERAPY OFCME
• Indicated when an inciting source of chronic CME can be defined and the edema fails
to respond to medical therapy
• Any retained lens fragments must be removed
• Nd:YAG laser vitreolysis or vitrectomy can be used to remove vitreous adhering to
cataract incision in order to relieve iris deformity or vitreomacular traction
• If IOL is mapositioned and contributing to chronic uveitis, repositioning or exchange
may be helpful
112.
DELAYED CHRONIC
ENDOPHTHALMITIS
• When;4 weeks to years; mean 9 months
• Caused by organisms of low virulence: e.g Propionibacterium acne or staph
epidermidis
113.
PSEUDOPHAKIC BULLOUS
KERATOPATHY
• Acontinuation of postop corneal edema produced by surgical or chemical insult to a
healthy or compromised corneal endothelium
• Common indication of penetrating keratoplasty
• RFs:
• -iris-dip lenses
• Closed-loop ACIOLs
• Fuchs corneal dystrophy
RETINAL DETACHMENT
• Higherincidence in aphakic patients than in phakic
• More common after ICCE than ECCE
• RFs:
• -vitreous loss after PCR
• -early onset PVD
• -associated myopia (AL>25mm)
• -younger age; male gender
• -lattice degeneration of retina
• Previous RD
• Plan: PPV +/- scleral buckle. Success rate: 85%
FIBROUS DOWNGROWTH
• Moreprevalent than epithelial ingrowth
• Happens when wound apposition is not perfect
• May cause:
• -secondary glaucoma
• -disorganization of anterior segment
• -phthisis bulbi
123.
AFTER CATARACT
• A.k.asecondary cataract
• Opacity which persists or develops after extracapsular cataract lens extraction
• Causes
• -residual opaque lens matter
• -proliferative type of after cataract can occur from the left-out anterior capsule
epithelial cells
124.
CLINICAL TYPES
• Maypresent as:
• -thickened posterior capsule
• -dense membranous after cataract
• -Soemmering’s ring: - a thick ring of after cataract formed behind the iris, enclosed
between the 2 layers of capsule
• -Elschnig’s pearls; here vacuolated subcapsular epithelial cells are clustered like soap
bubbles along the posterior capsule.
125.
TREATMENT
• Thin membranousafter cataract and thickened posterior capsule are best treated by
YAG-laser capsulotomy or dissection with cystitome or Zeigler’s knife
• Dense membranous after cataract needs surgical membranectomy
• Soemmering’s ring after cataract with clean central posterior capsule needs no
treatment
• Elschnig’s pearls involving the central part of the posterior capsule can be treated with
YAG-laser capsulotomy or discussion with cystitome.
GLAUCOMA-IN-APHAKIA AND
PSEUDOPHAKIA
• 1)Raised IOP with deep anterior chamber in early postoperative period
• Due to:
• -hyphema
• -inflammation
• -retained cortical matter or vitreous filling the AC
• 2) Secondary angle-closure glaucoma due to flat AC:
• -Following long-standing wound leak
• 3)Secondary angle-closure glaucoma due to pupil block:
• -Following annular synechiae or vitreous herniation
128.
.• 4) Undiagnosedpreexisting primary open-angle glaucoma
• 5) steroid-induced glaucoma
• -due to postop corticosteroids after cataract surgery
• 6) epithelial ingrowth
• 7) aphakic/pseudophakic malignant glaucoma
IOL RELATED COMPLICATIONS
•1) CME
• 2) UGH syndrome
• 3) Malposition of IOL
• 4) Pupillary capture of the IOL
• 5) TASS
131.
UGH (ELLINGSON SYNDROME)
•Concurrent occurrence of uveitis, glaucoma and hyphema
• First described in context of rigid or closed-loop ACIOLs
• Causes:
• -inappropriate IOL sizing
• -contact between the implant and vascular structures or the corneal endothelium
• -defects in implant manufacturing
• Medical treatment:
• -cycloplegics
• -topical anti-inflammatory
• -ocular hypotensive medications
132.
SURGICAL APPROACH
• Indication:
•-If medical therapy does not sufficiently address the findings
• -If inflammation threatens either retinal or corneal function
• To do: IOL removal
• -Challenge: inflammatory scars, esp in the AC angle or posterior to iris
• -Solution: amputate the haptics from the optic and remove the lens piecemeal,
• -rotating the haptic material out of the synechial tunnels to minimize trauma to eye
• In some cases, it is safer to leave portions of the haptics in place
• Early lens explantation may reduce the risk of corneal decompression and CME
133.
MALPOSITION OF IOL
•Inform of:
• -decentration
• -subluxation
• -dislocation
• Some fancy names:
• -sunset syndrome (inferior subluxation of IOL)
• -sunrise syndrome (superior subluxation of IOL)
• -Lost lens syndrome: -complete dislocation of an IOL into the vitreous cavity
• -Windshield wiper syndrome:
-occurs when a very small IOL is placed vertically in the sulcus.
-in this the superior loop moves to the left and right, with movements of the head