Downloaded 200 times


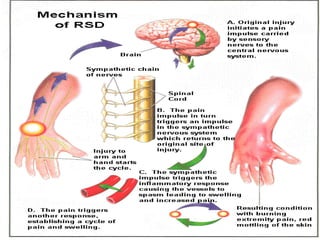
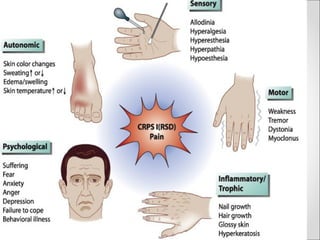







This document discusses complex regional pain syndrome (CRPS), formerly known as reflex sympathetic dystrophy. It defines CRPS as a multi-symptom syndrome that usually affects one or more extremities and is characterized by disproportionate pain, vasomotor instability, trophic skin changes, and regional osteoporosis. Trauma is a common precipitating factor. Management involves a multidisciplinary approach including physical therapy, medications to relieve symptoms, and in some cases surgical or injection-based treatments.






























































![CRPS ppt sajad final final [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/crpspptsajadautosaved-250921194258-ec8857be-thumbnail.jpg?width=640&height=640&fit=bounds)






























![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











