Downloaded 20 times




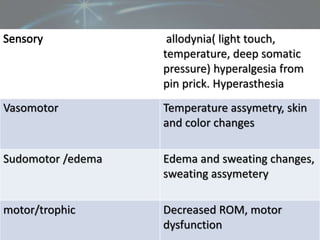




Reflex Sympathetic Dystrophy (RSD), also known as Complex Regional Pain Syndrome (CRPS), is a chronic condition that causes persistent burning pain, swelling, and abnormal nerve activity in an affected limb, usually following an injury. It has two types: RSD (type I) occurs without major nerve damage and Causalgia (type II) occurs due to nerve injury. Symptoms include allodynia, hyperalgesia, changes in skin temperature and color. Diagnosis involves assessing sensory, vasomotor, sudomotor and motor symptoms. Treatment includes medications, surgery such as sympathectomy, and physiotherapy involving exercises, massage, and splinting to relieve pain and edema.











































![COMPLEX REGIONAL PAIN SYNDROME [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/complexregionalpainsyndromeautosaved-240617174113-5512c3fe-thumbnail.jpg?width=640&height=640&fit=bounds)











































