Downloaded 800 times
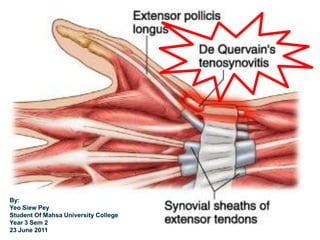

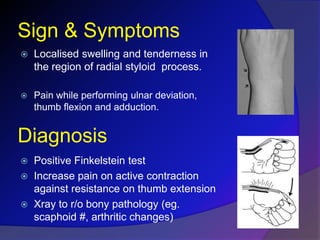
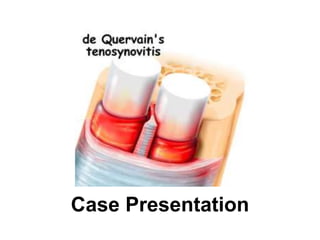


De Quervain's disease is a stenosing tenosynovitis of the first dorsal compartment of the wrist caused by inflammation of the tendon sheaths of the abductor pollicis longus and extensor pollicis brevis tendons. It often affects women ages 30-50 and is caused by repetitive motions of the thumb like gripping. Symptoms include pain on the radial side of the wrist worsened by ulnar deviation and thumb movement. Diagnosis is based on tenderness over the tendon sheaths and a positive Finkelstein's test. Most cases are treated conservatively with splinting, activity modification and anti-inflammatories while surgery is reserved for persistent cases.





















































































