Downloaded 465 times


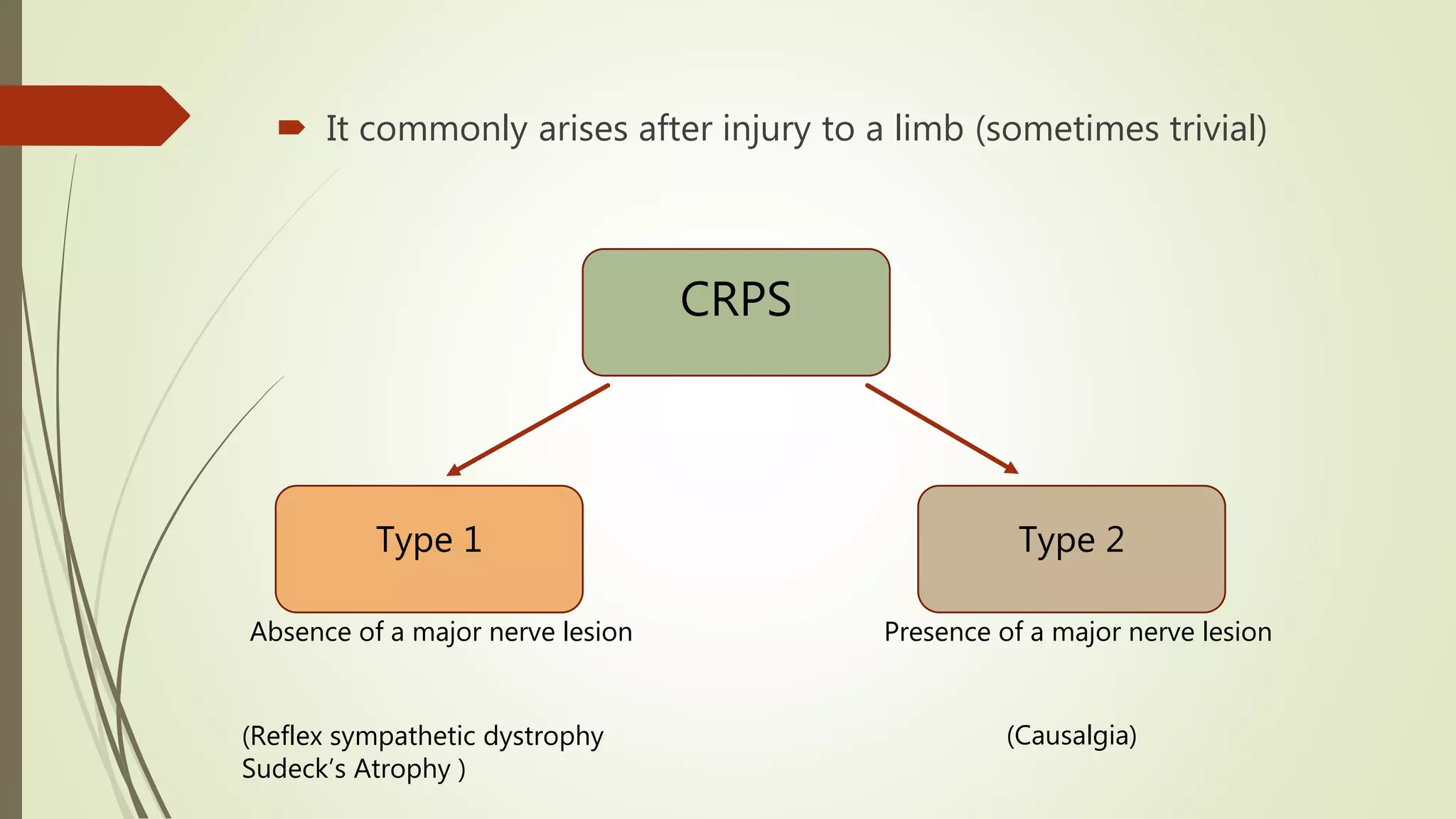












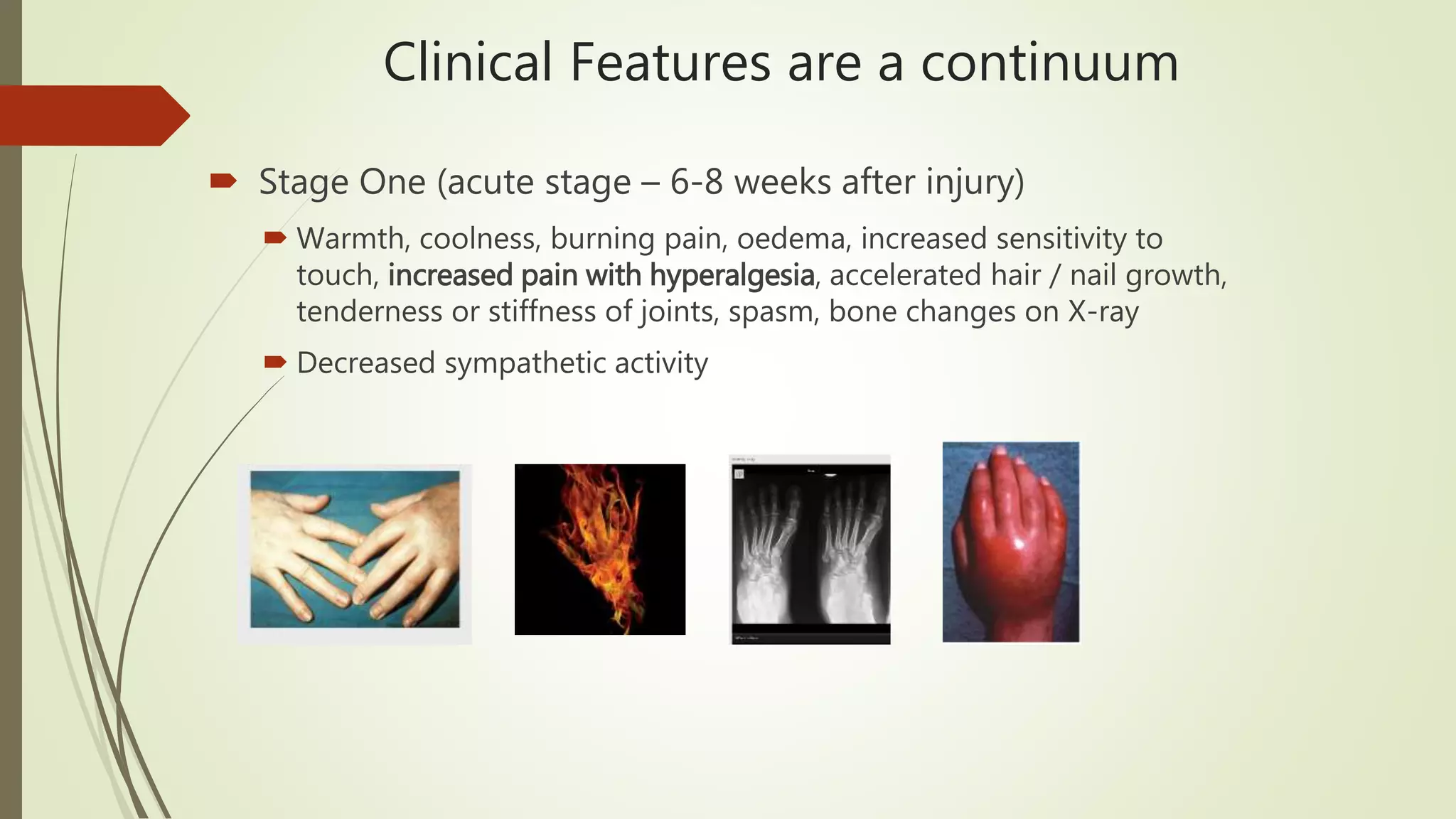
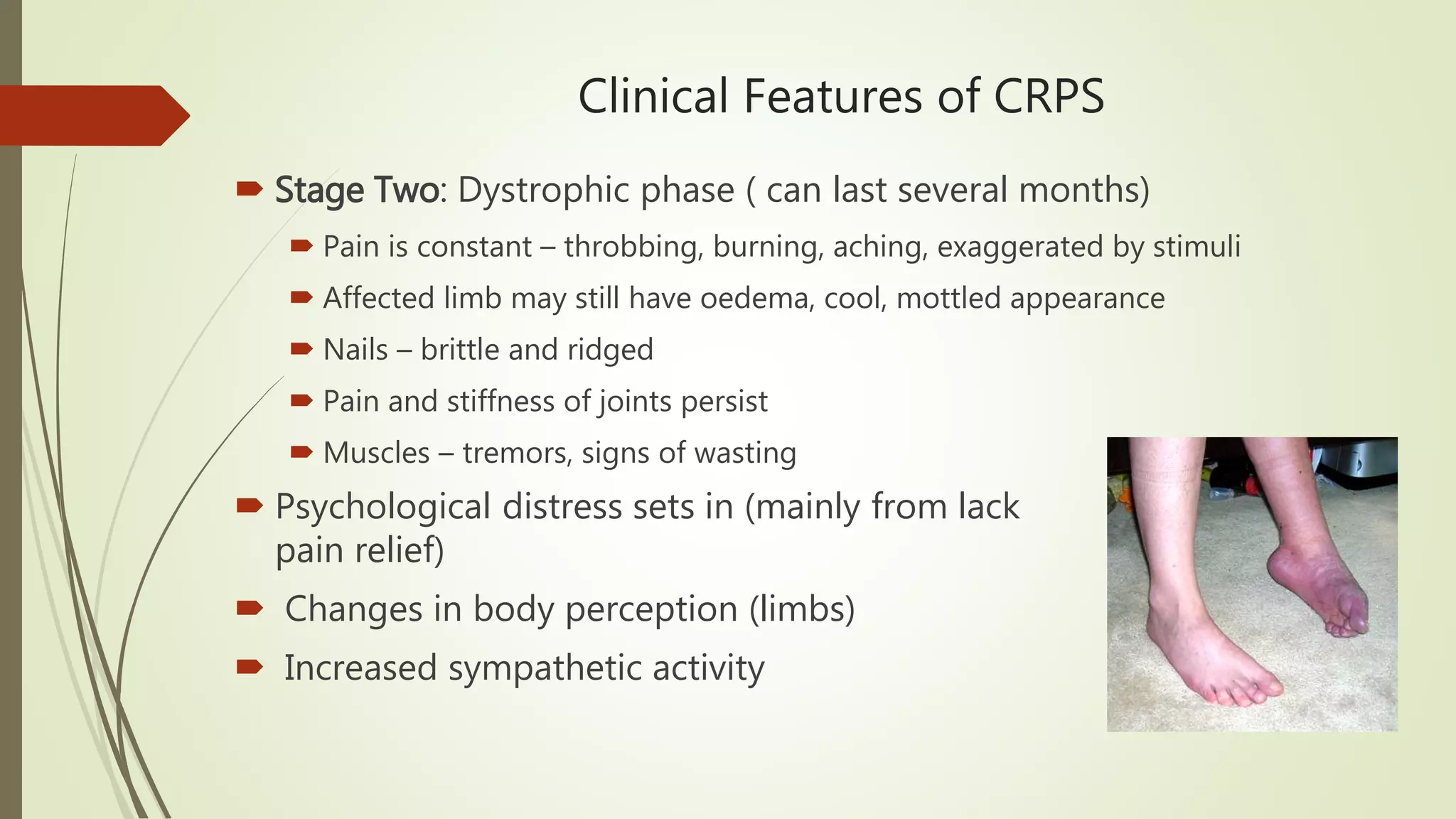
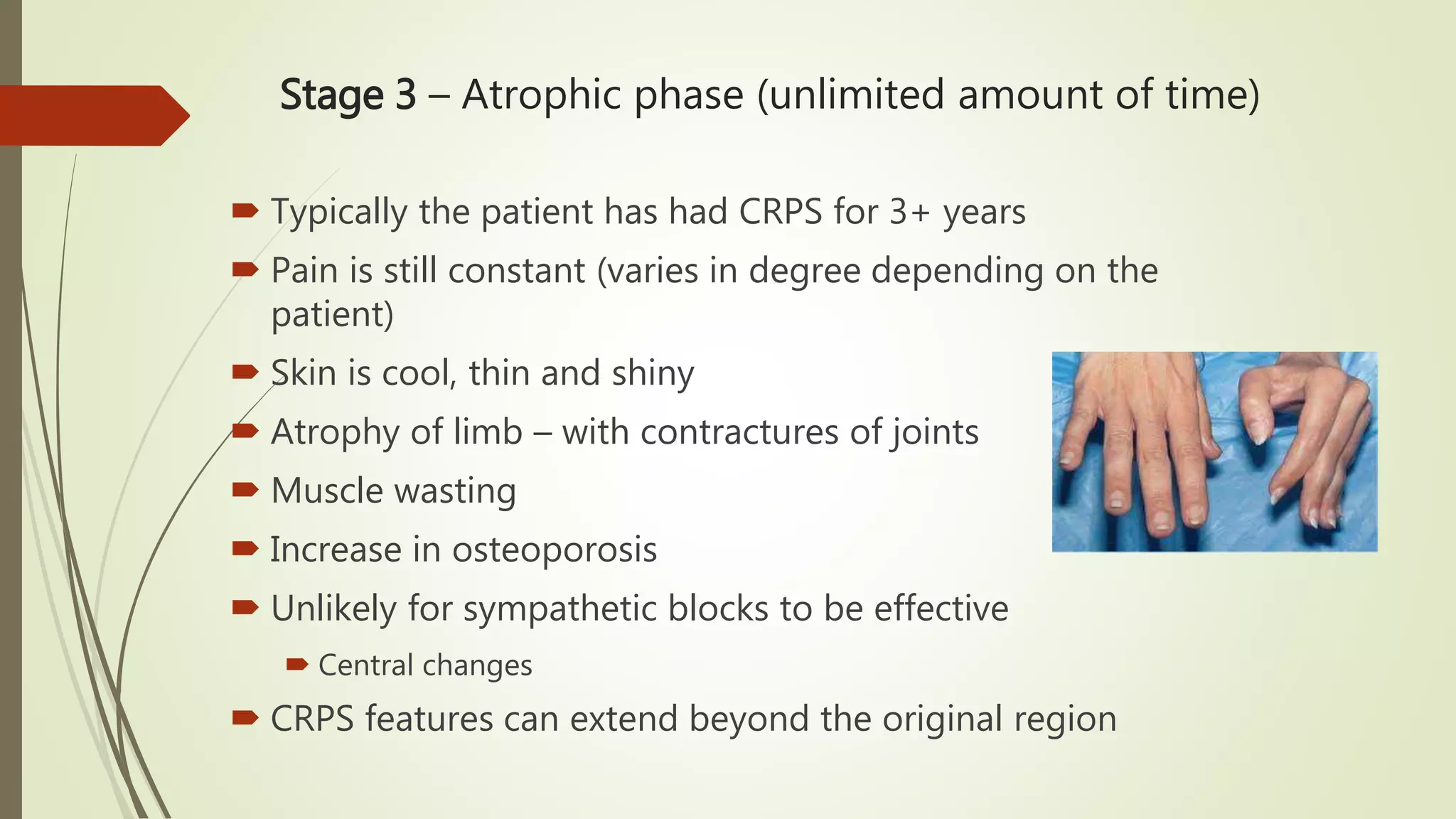






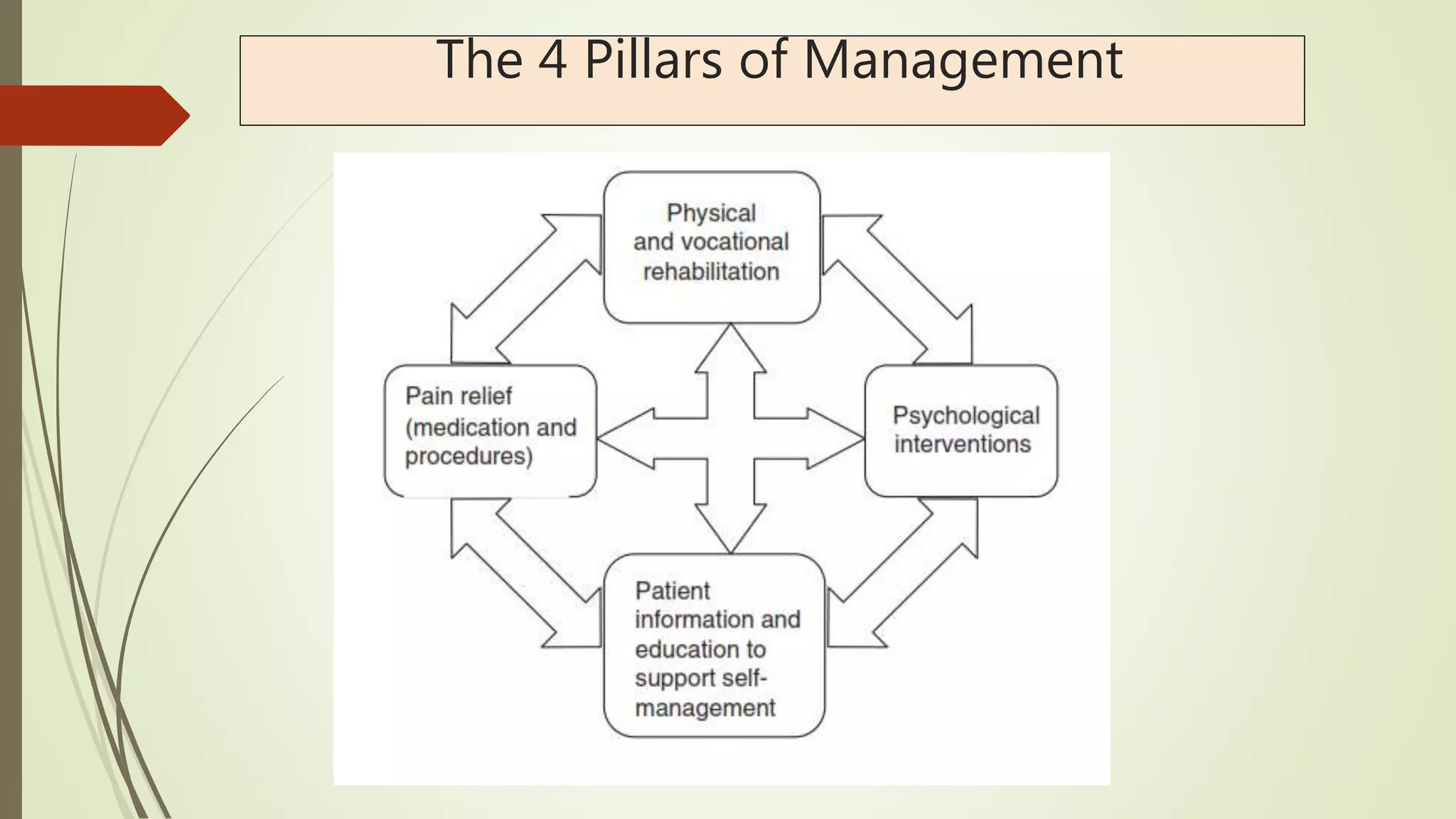

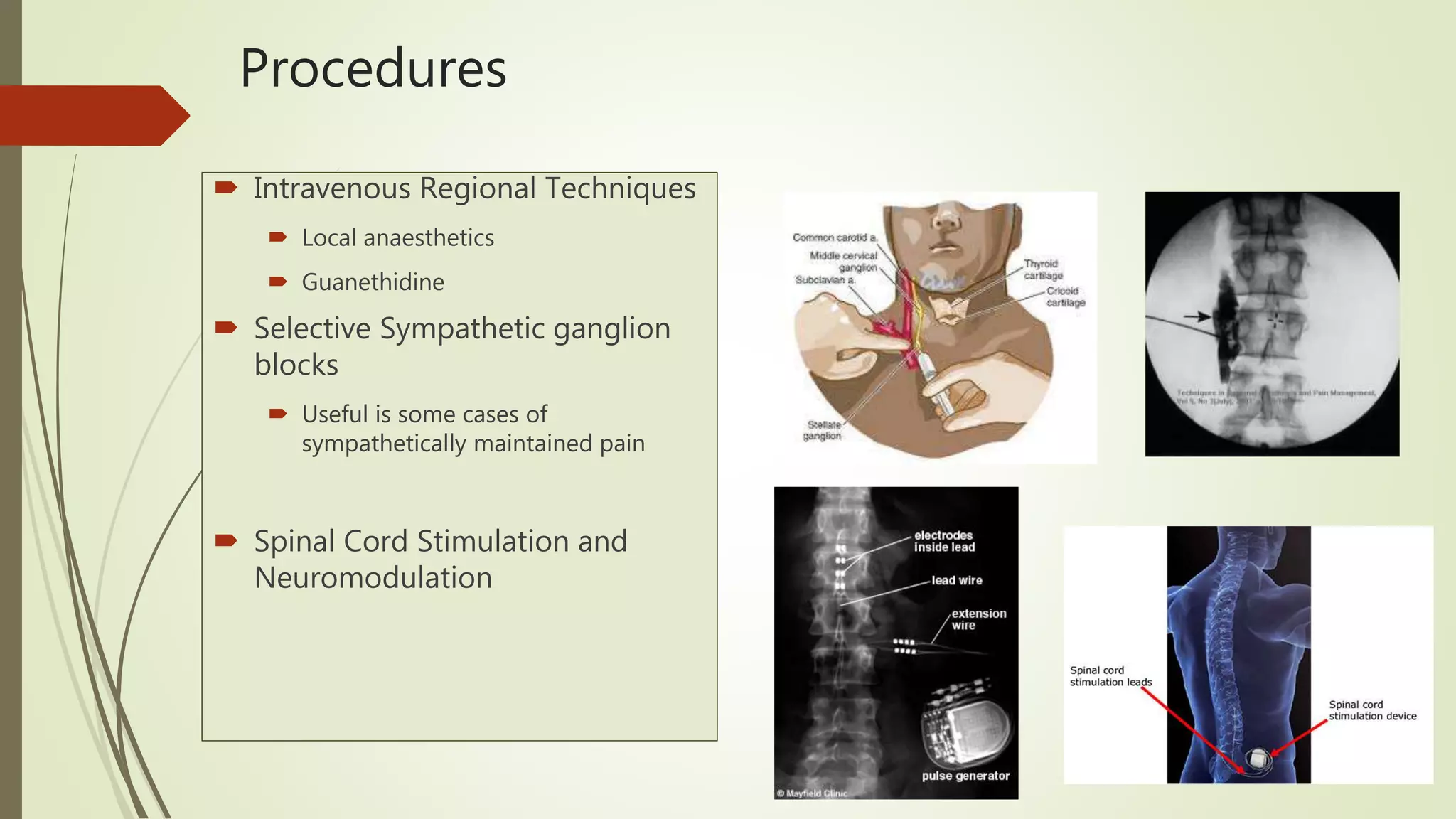
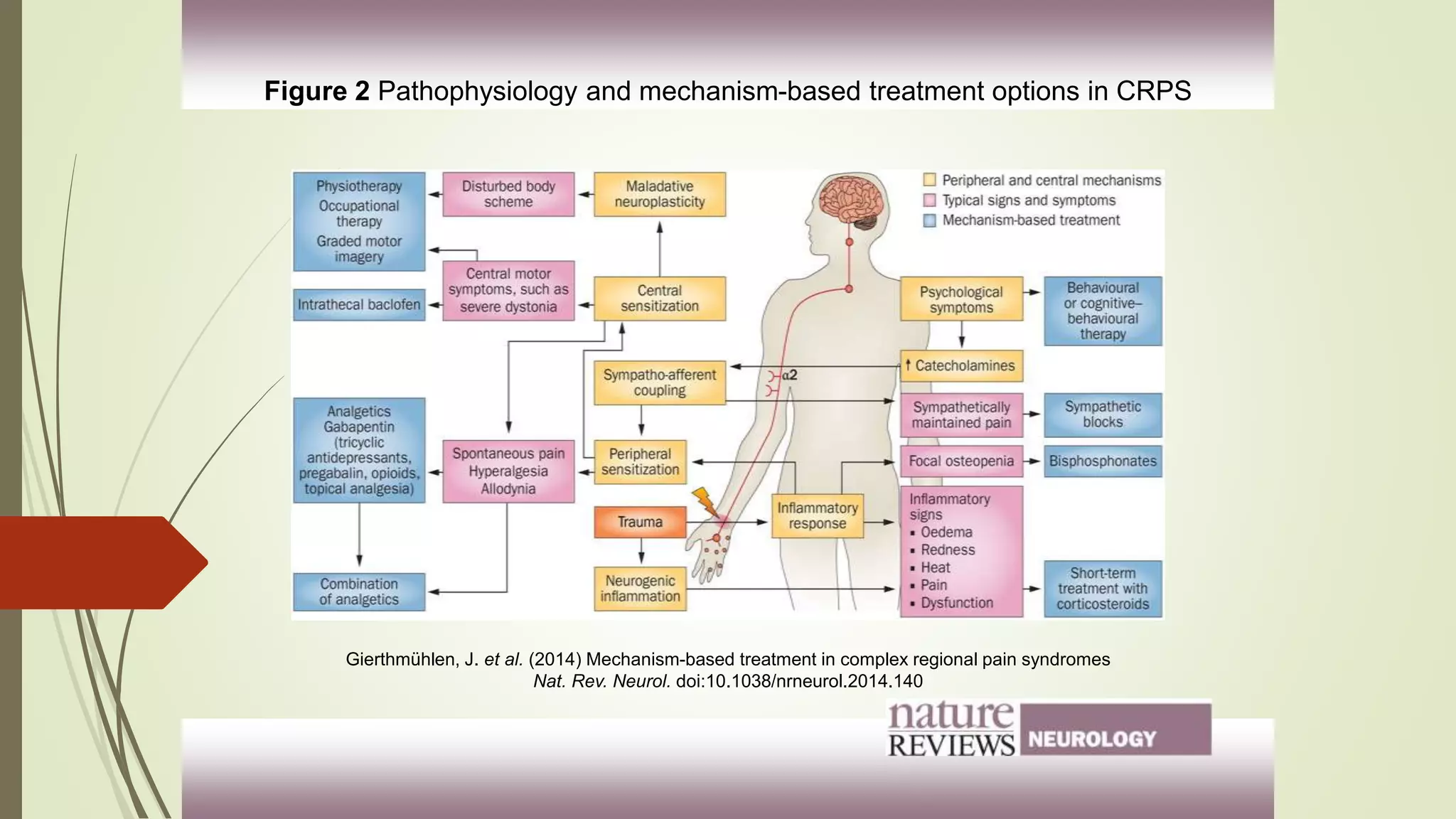
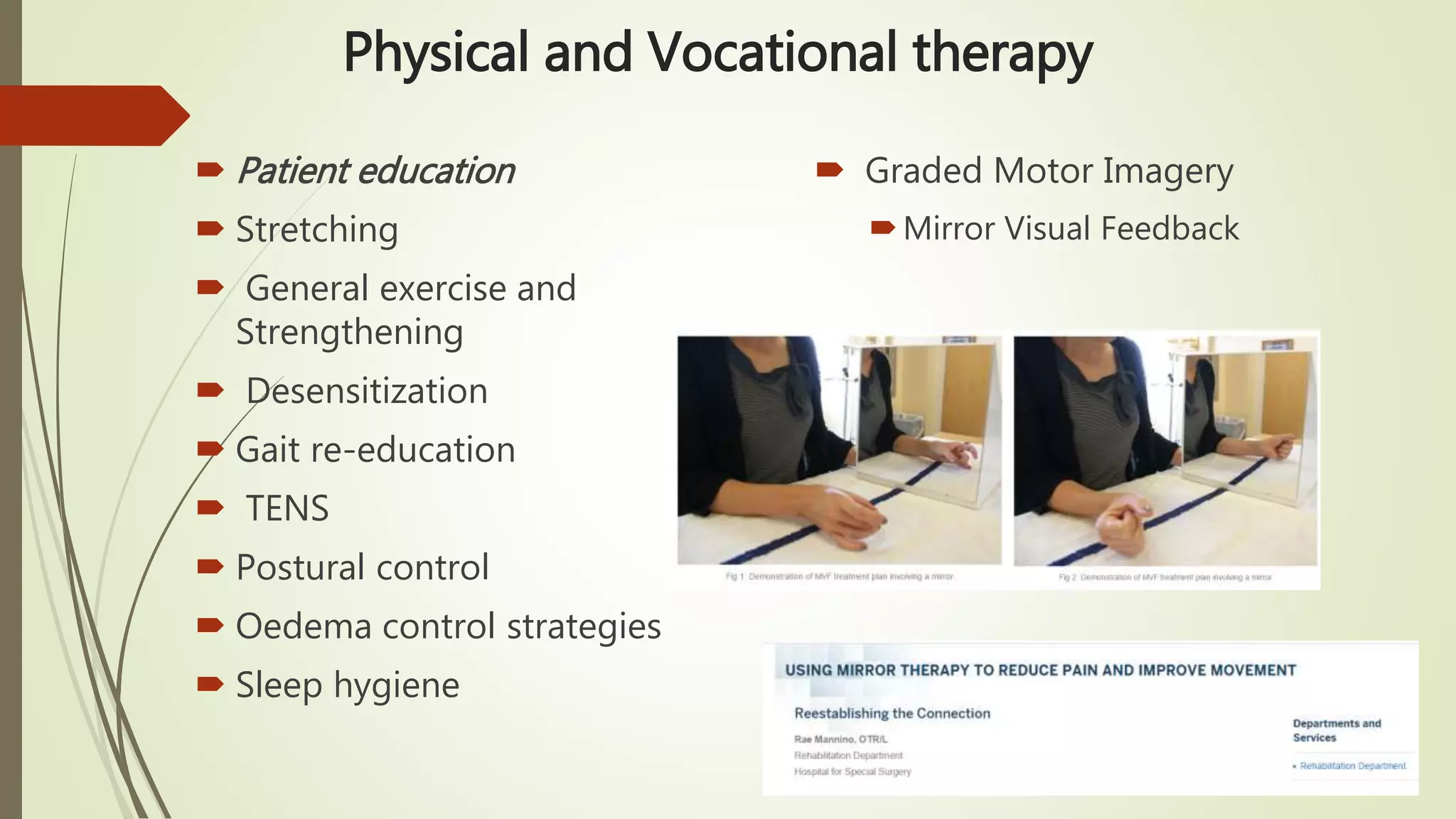






Complex Regional Pain Syndrome (CRPS) is a debilitating painful condition affecting a limb. It is associated with sensory, motor, autonomic, skin and bone abnormalities. The leading symptom is pain, which is often associated with limb dysfunction and psychological distress. CRPS arises after an injury to a limb and is classified into two types depending on whether there is a major nerve lesion present. Management involves a multidisciplinary approach with four pillars - pain relief through medications, procedures, physical and vocational therapy, and psychological therapy. Early diagnosis and treatment are important to help patients.



































![COMPLEX REGIONAL PAIN SYNDROME [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/complexregionalpainsyndromeautosaved-240617174113-5512c3fe-thumbnail.jpg?width=640&height=640&fit=bounds)











![CRPS ppt sajad final final [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/crpspptsajadautosaved-250921194258-ec8857be-thumbnail.jpg?width=640&height=640&fit=bounds)

























