Downloaded 268 times
![Definition
Head injury / Traumatic brain injury
◦ “any alteration in mental or physical functioning related
to a blow to the head”
◦ “Loss of consciousness does not need to occur”
source: David A Olson. Head injury [internet] 2013 [updated Apr 1 2013] available from
http://emedicine.medscape.com/article/1163653](https://image.slidesharecdn.com/qye2wrnssqsw64fz1ayf-signature-b051517d44d5bc61335748b5f2c057a2109e8dc7e8f535f7acce5e6bc85bc39b-poli-150801154502-lva1-app6892/85/Head-injury-finalized-4-320.jpg)


![References
• David A Olson. Head injury [internet] 2013 [updated Apr 1 2013] available from
http://emedicine.medscape.com/article/1163653
• Principle and practice of Surgery 5th Edition, O. James Garden
• Anderson P. Hemodynamic Complications Common in Traumatic Brain Injury.
Available at http://www.medscape.com/viewarticle/778999. Accessed March 25,
2013.
• Eisenberg HM, Gary HE Jr, Aldrich EF, et al. Initial CT findings in 753 patients with
severe head injury. A report from the NIH Traumatic Coma Data Bank. J Neurosurg.
Nov 1990;73(5):688-98.
• Mark S. Greenberg MD, Handbook of Neurosurgery 7th edition
• NICE clinical guideline 176 guidance.nice.org.uk/cg176. Triage, assessment,
investigation and early management of head injury in children, young people and
adults (Issued: January 2014)](https://image.slidesharecdn.com/qye2wrnssqsw64fz1ayf-signature-b051517d44d5bc61335748b5f2c057a2109e8dc7e8f535f7acce5e6bc85bc39b-poli-150801154502-lva1-app6892/85/Head-injury-finalized-57-320.jpg)

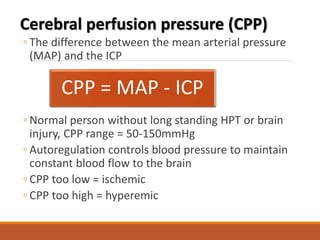
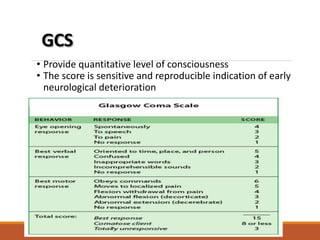
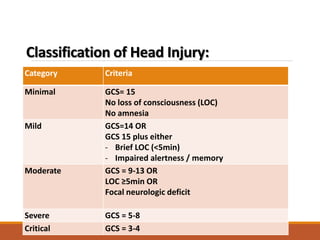
Head injuries can range from mild to severe based on factors like loss of consciousness and Glasgow Coma Scale. The primary goals of management are to stabilize the patient by protecting the airway and maintaining adequate oxygenation, ventilation, and circulation to prevent secondary brain injury. Imaging with CT scan is important to identify fractures and intracranial bleeding like extradural and subdural hematomas that may require neurosurgery. Ongoing monitoring of things like neurological status and intracranial pressure is also important for managing head injuries.























































































