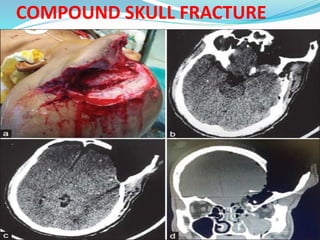
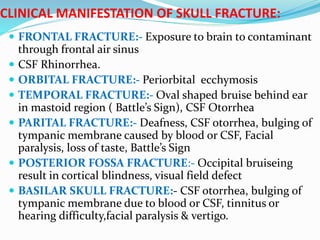
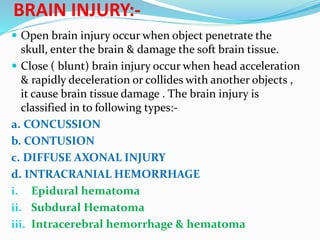
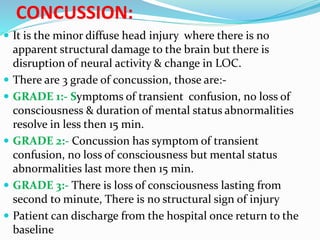
This document provides information on head injuries including traumatic brain injury. It discusses the types of head injuries such as scalp lacerations, skull fractures, and various types of brain injuries including concussions, contusions, diffuse axonal injuries, and intracranial hemorrhages. The etiology, signs and symptoms, diagnosis, management including surgery if needed, and nursing care are described for different head injury types.


































![5 Head injury (1)[1]_425974386d4d442b6ce092649f8d5b41.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/5headinjury11425974386d4d442b6ce092649f8d5b41-250318200004-e6284666-thumbnail.jpg?width=640&height=640&fit=bounds)
![5 Head injury (1)[1]_425974386d4d442b6ce092649f8d5b41.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/5headinjury11425974386d4d442b6ce092649f8d5b41-250319190324-4867f9fb-thumbnail.jpg?width=640&height=640&fit=bounds)
























































