Downloaded 149 times
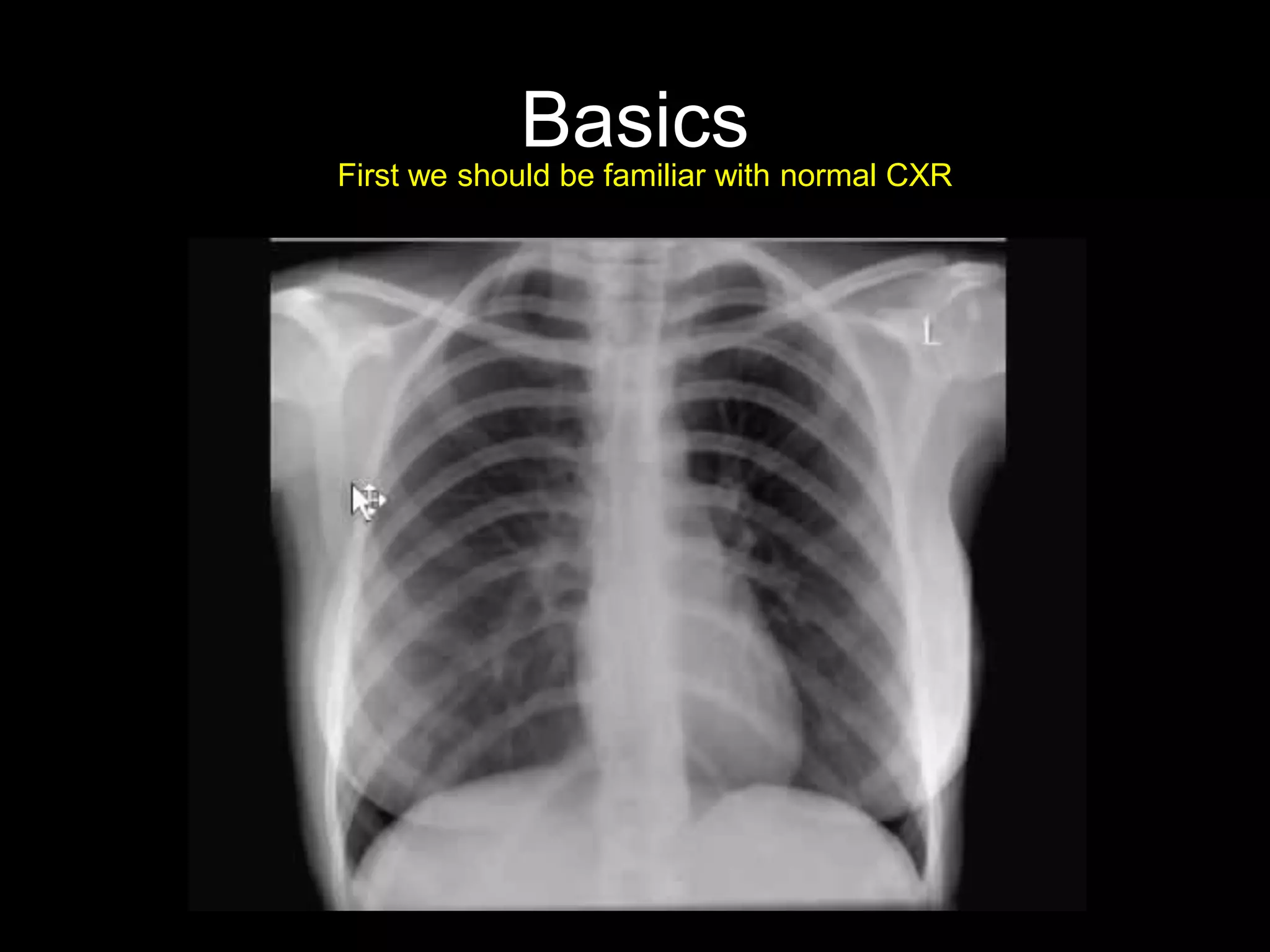
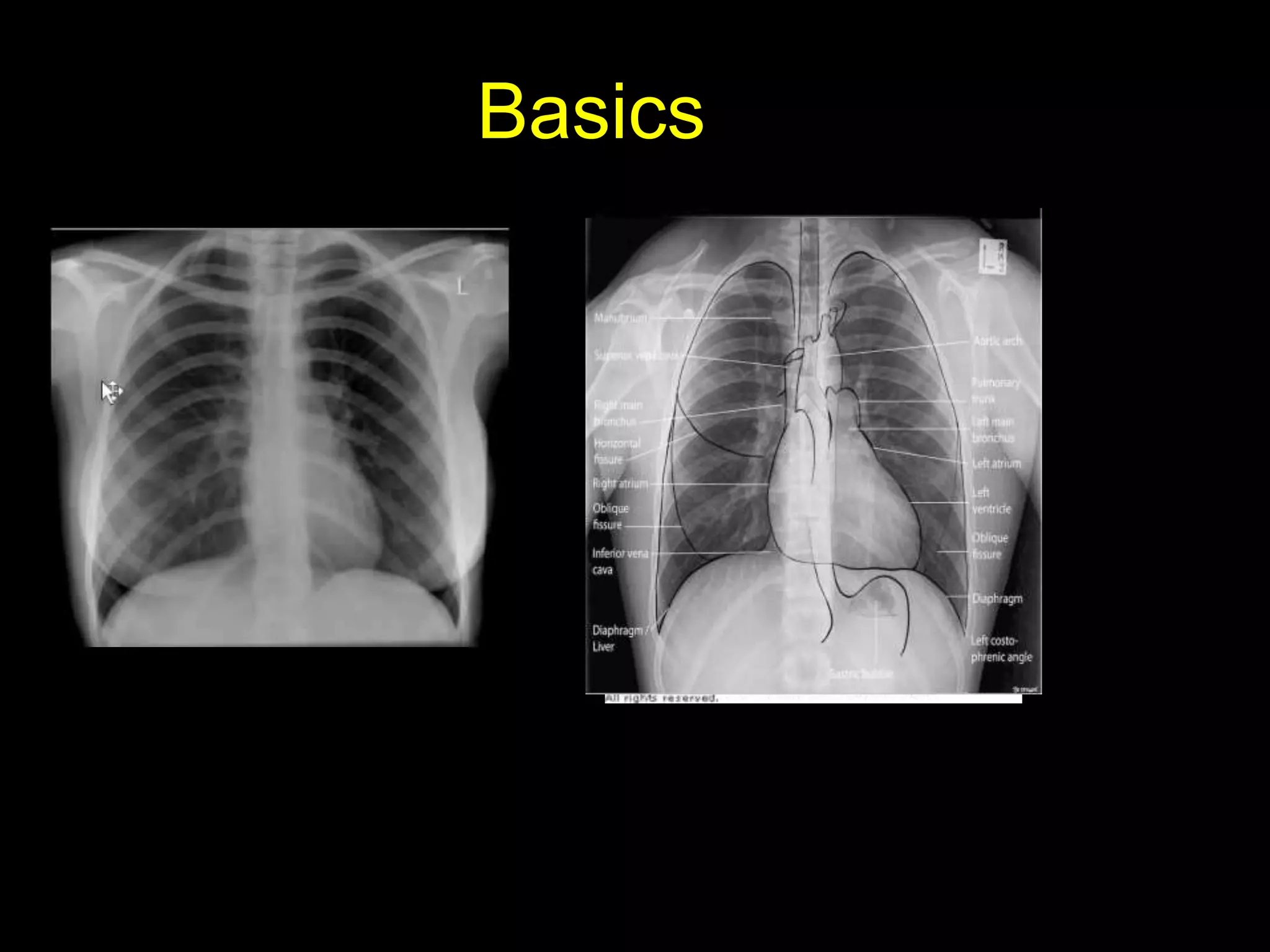
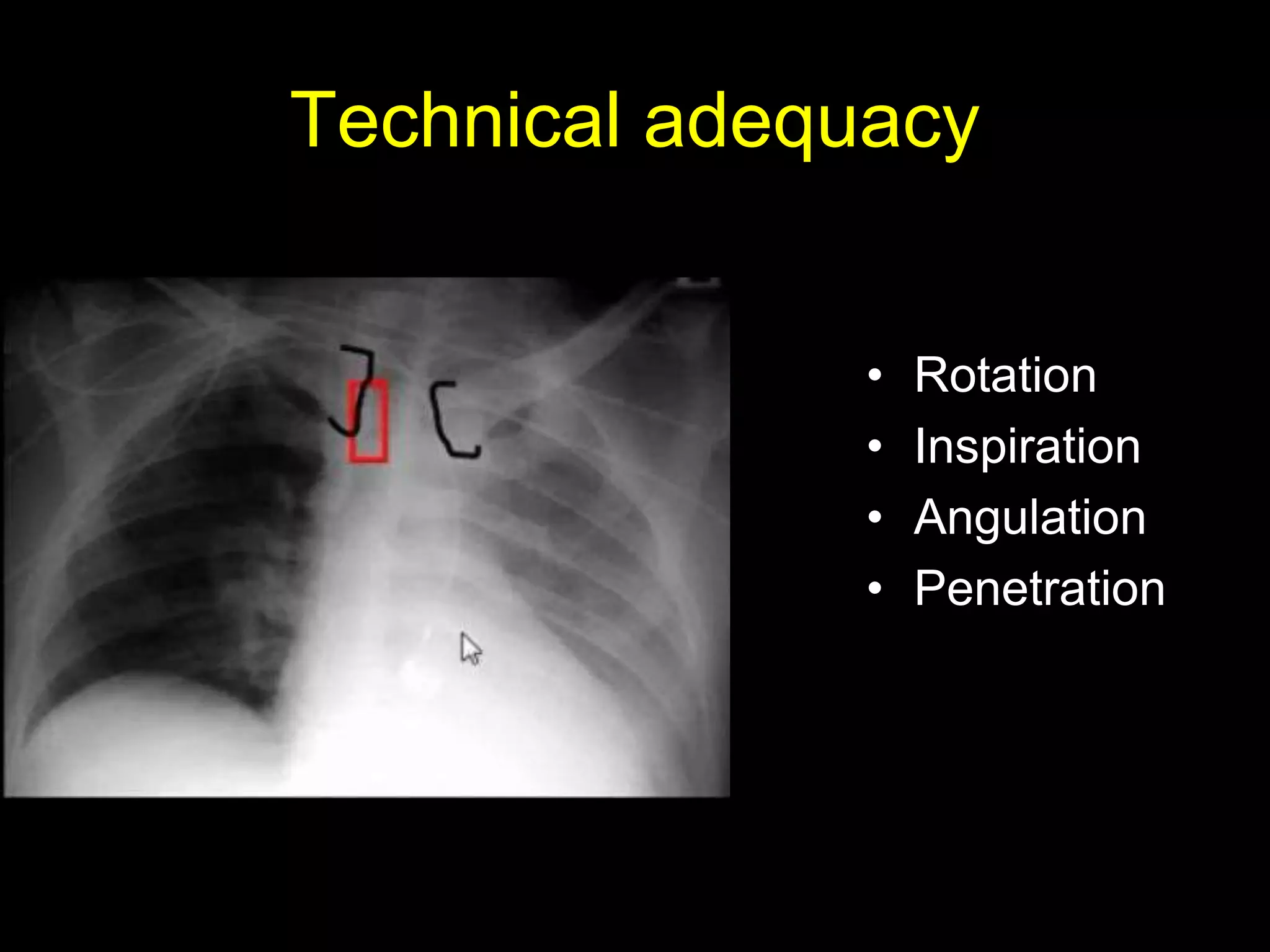
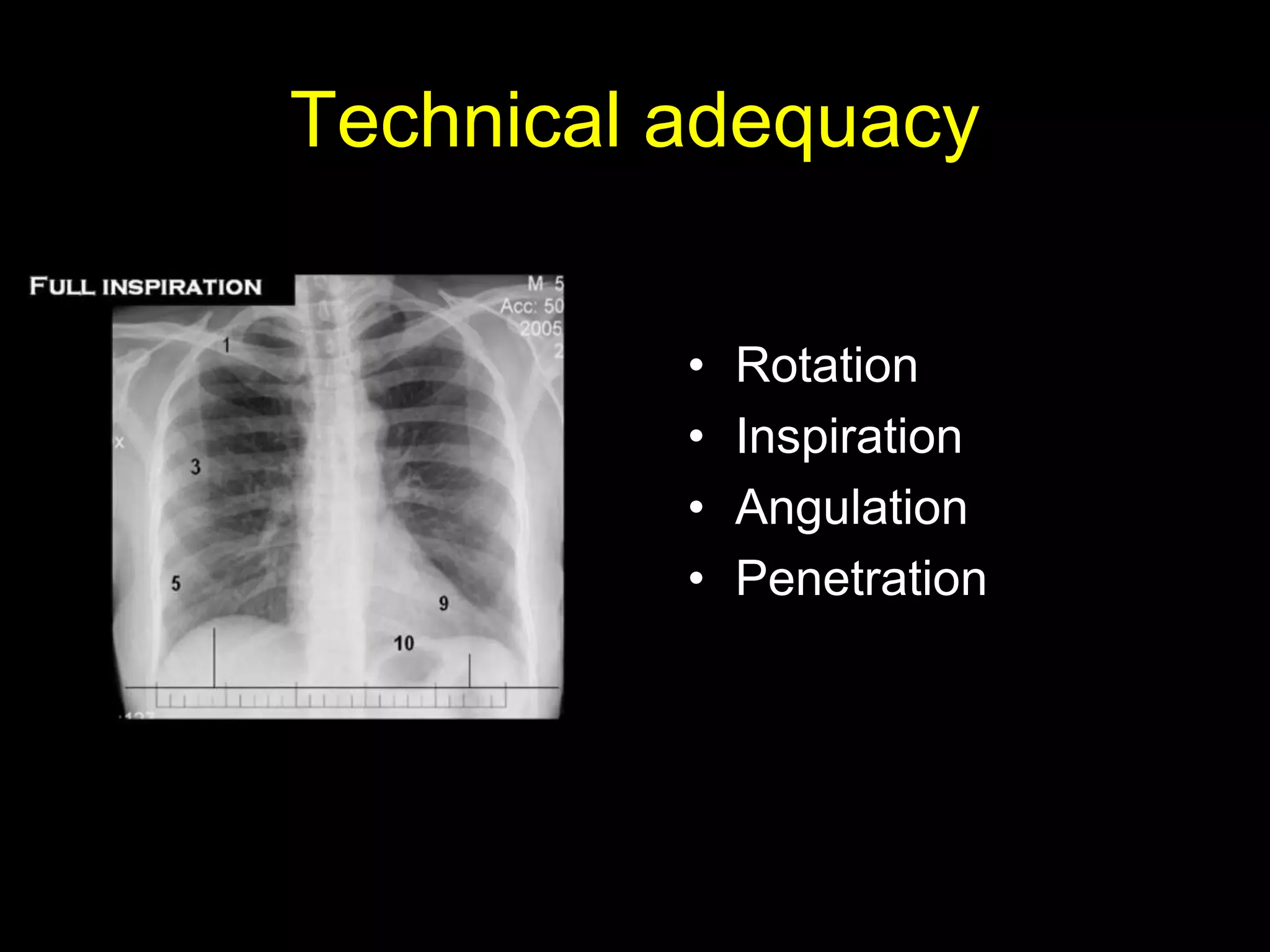
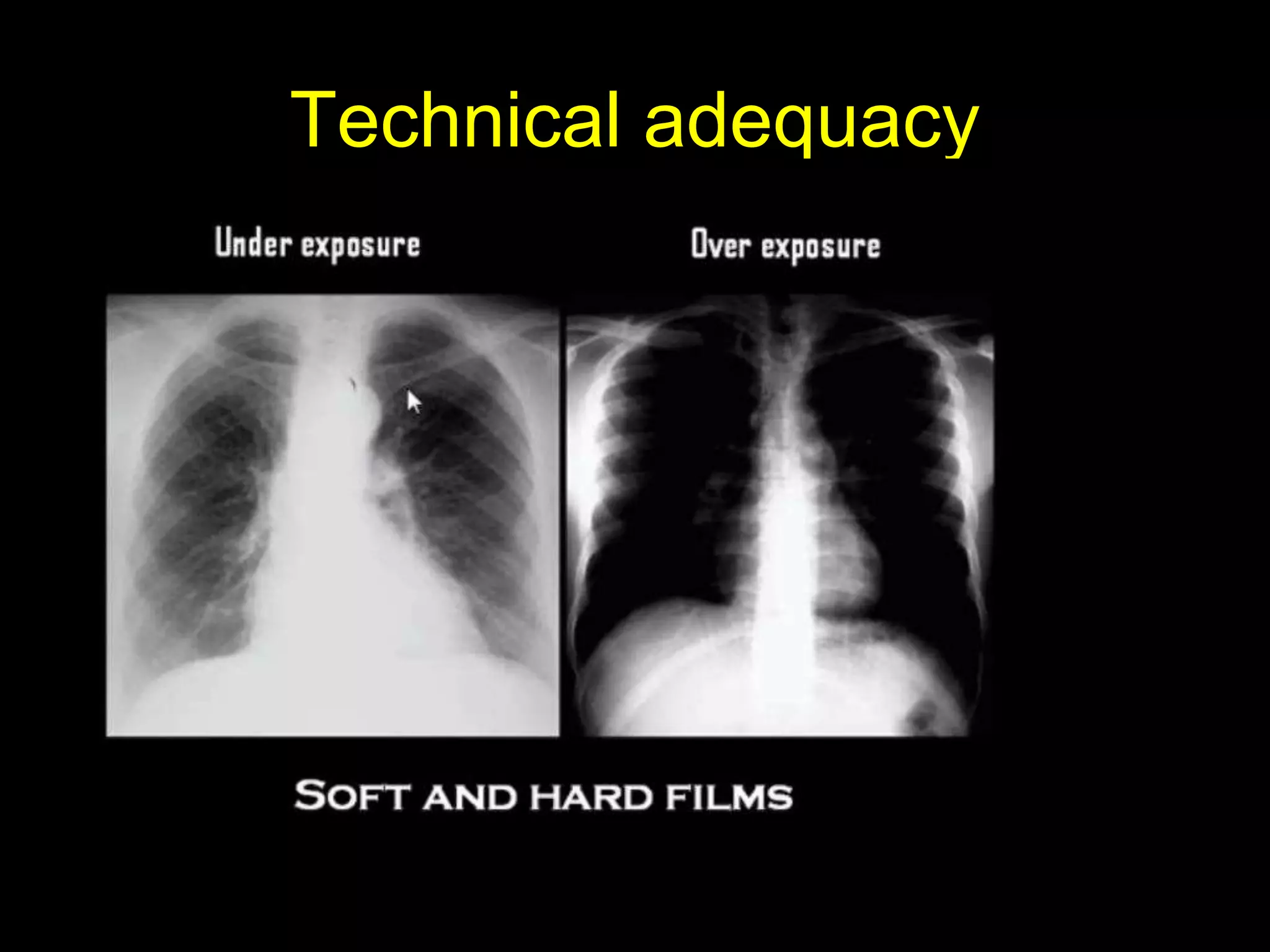
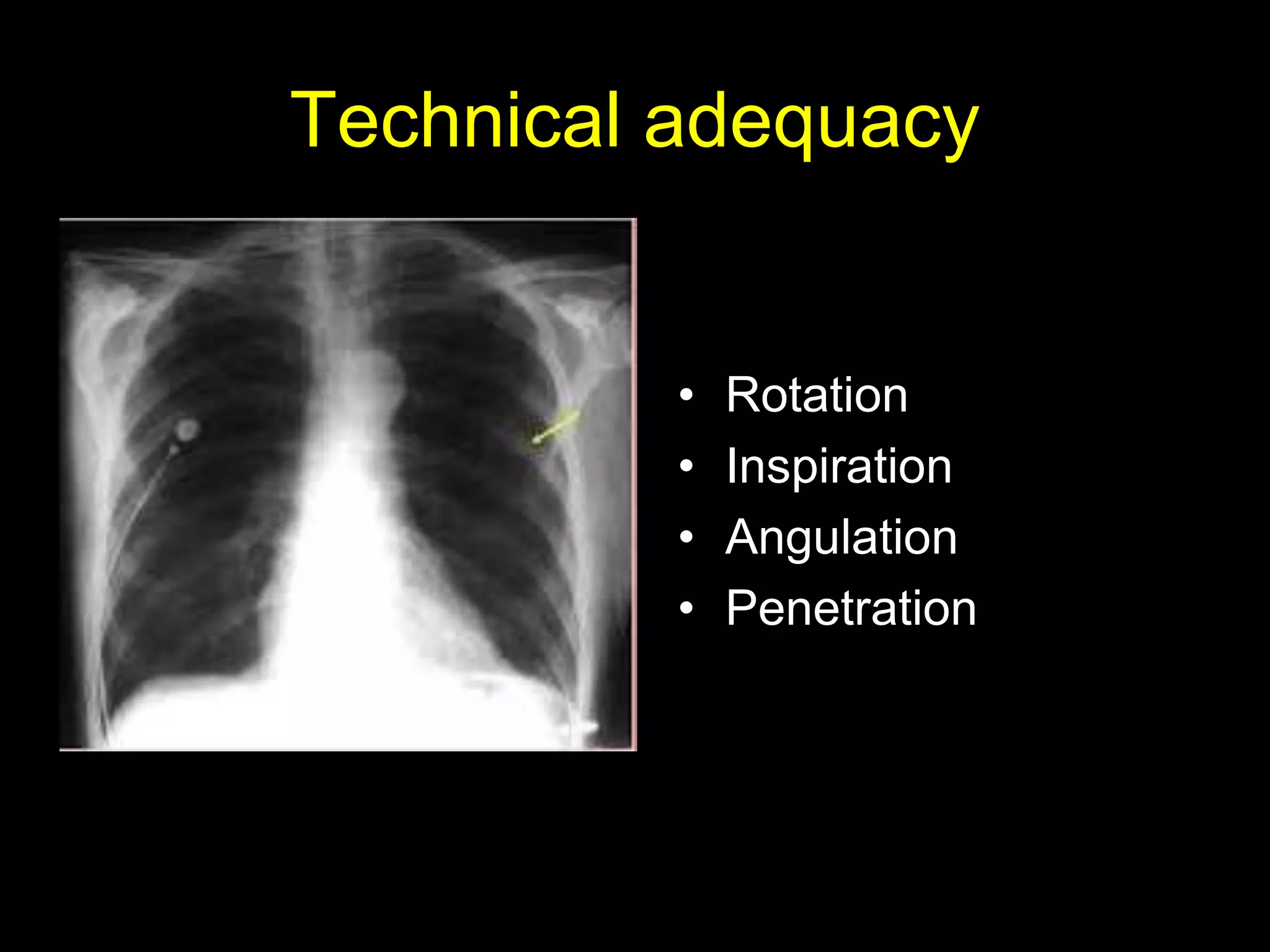
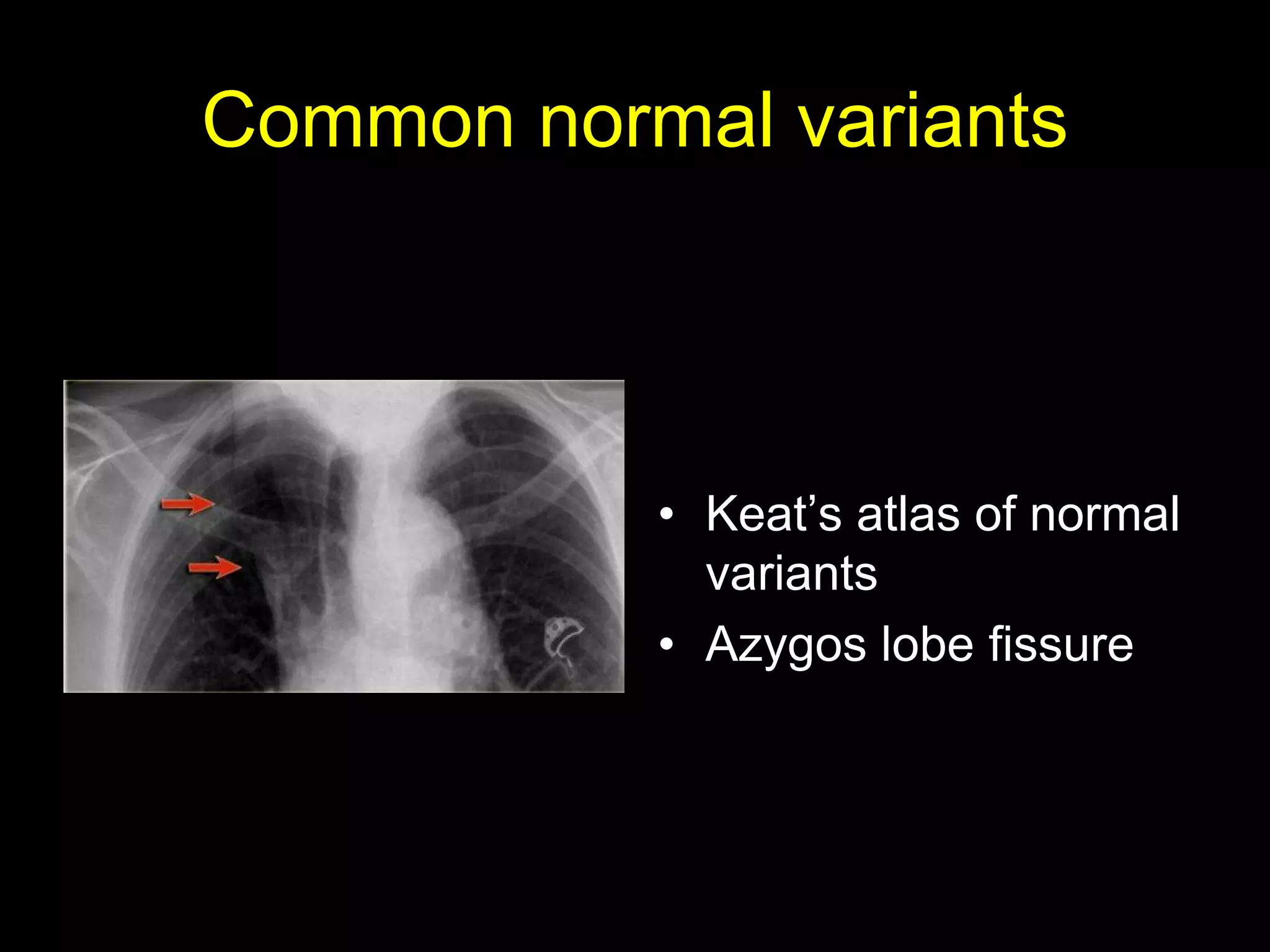
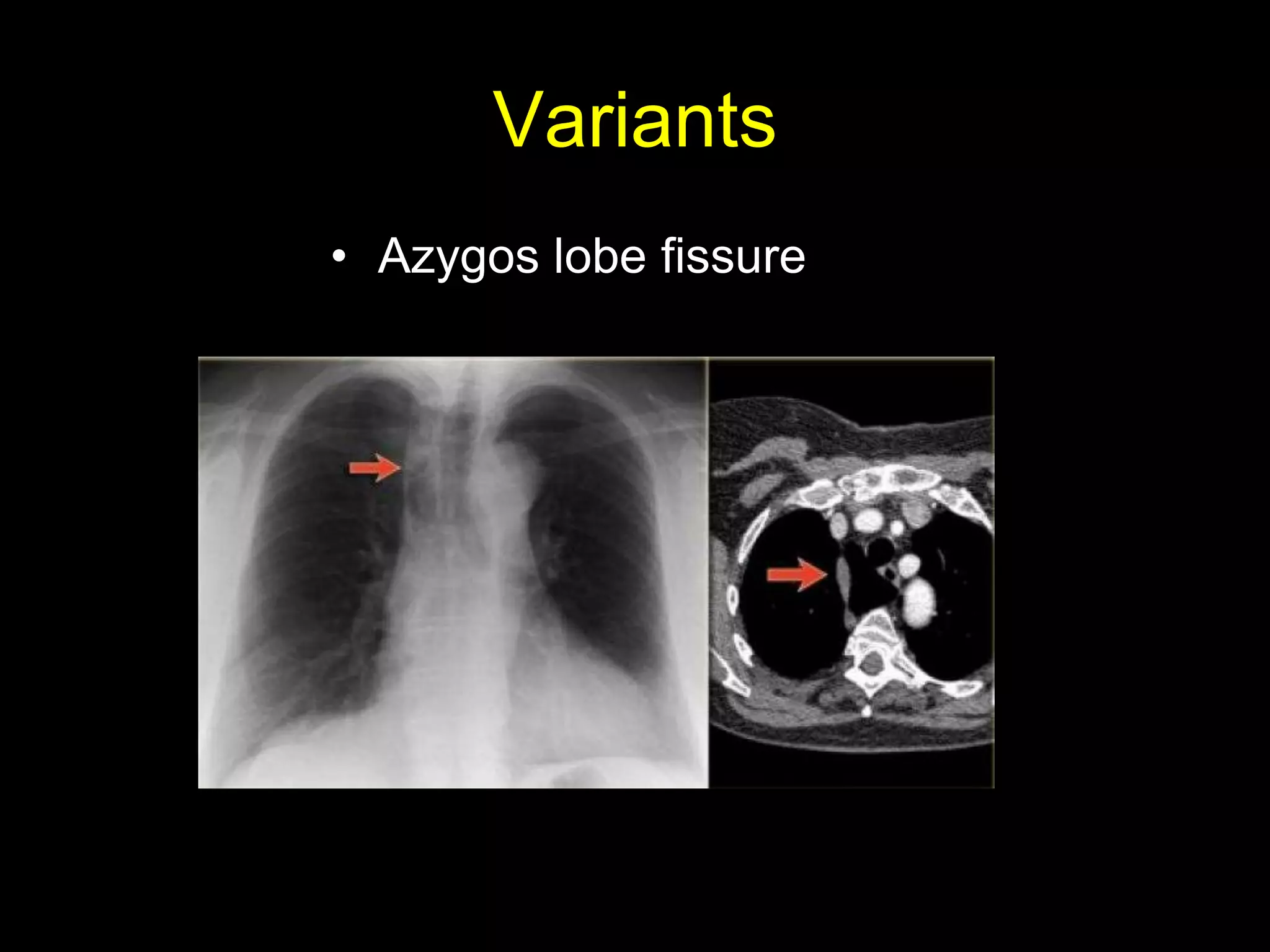
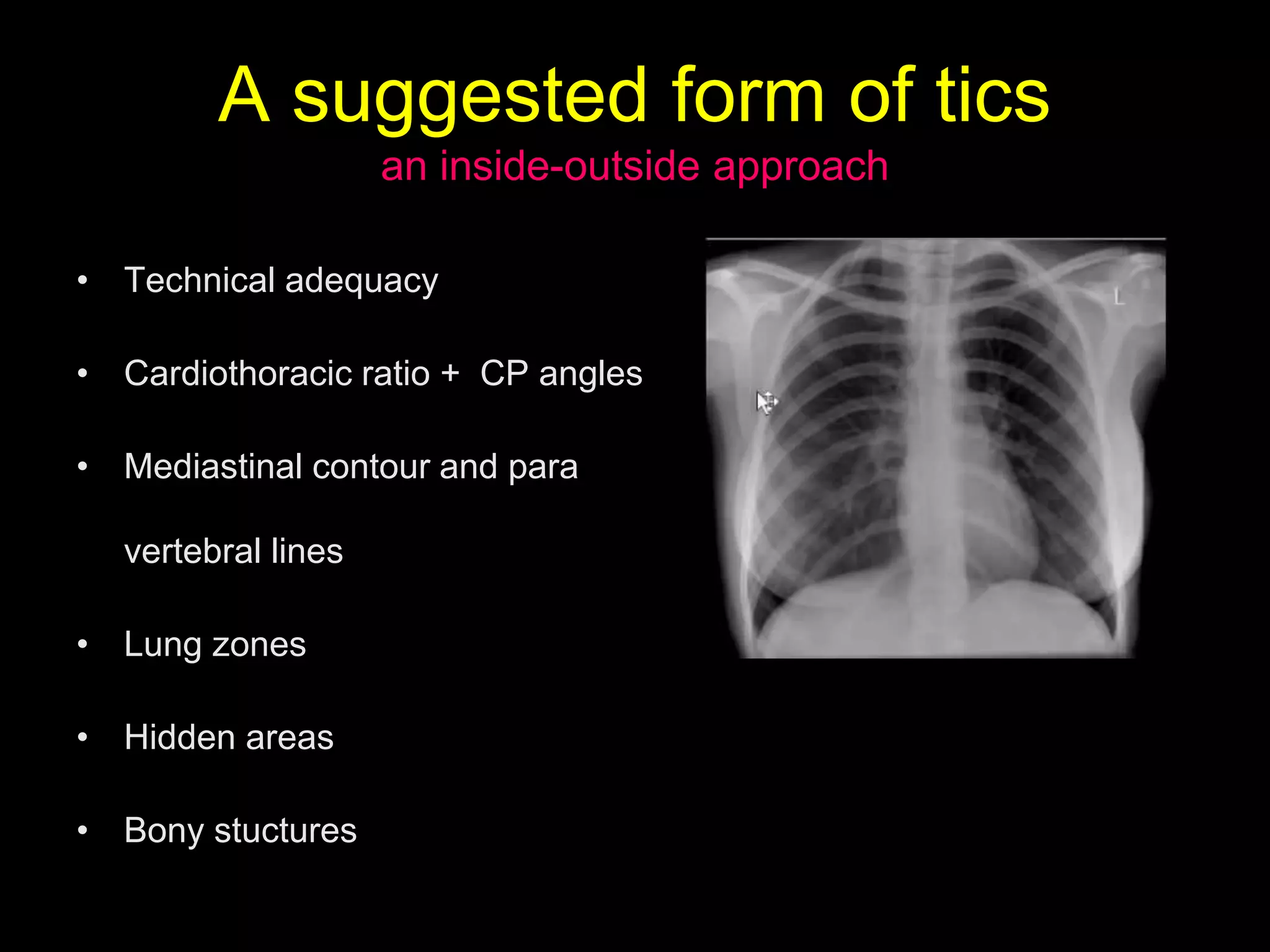
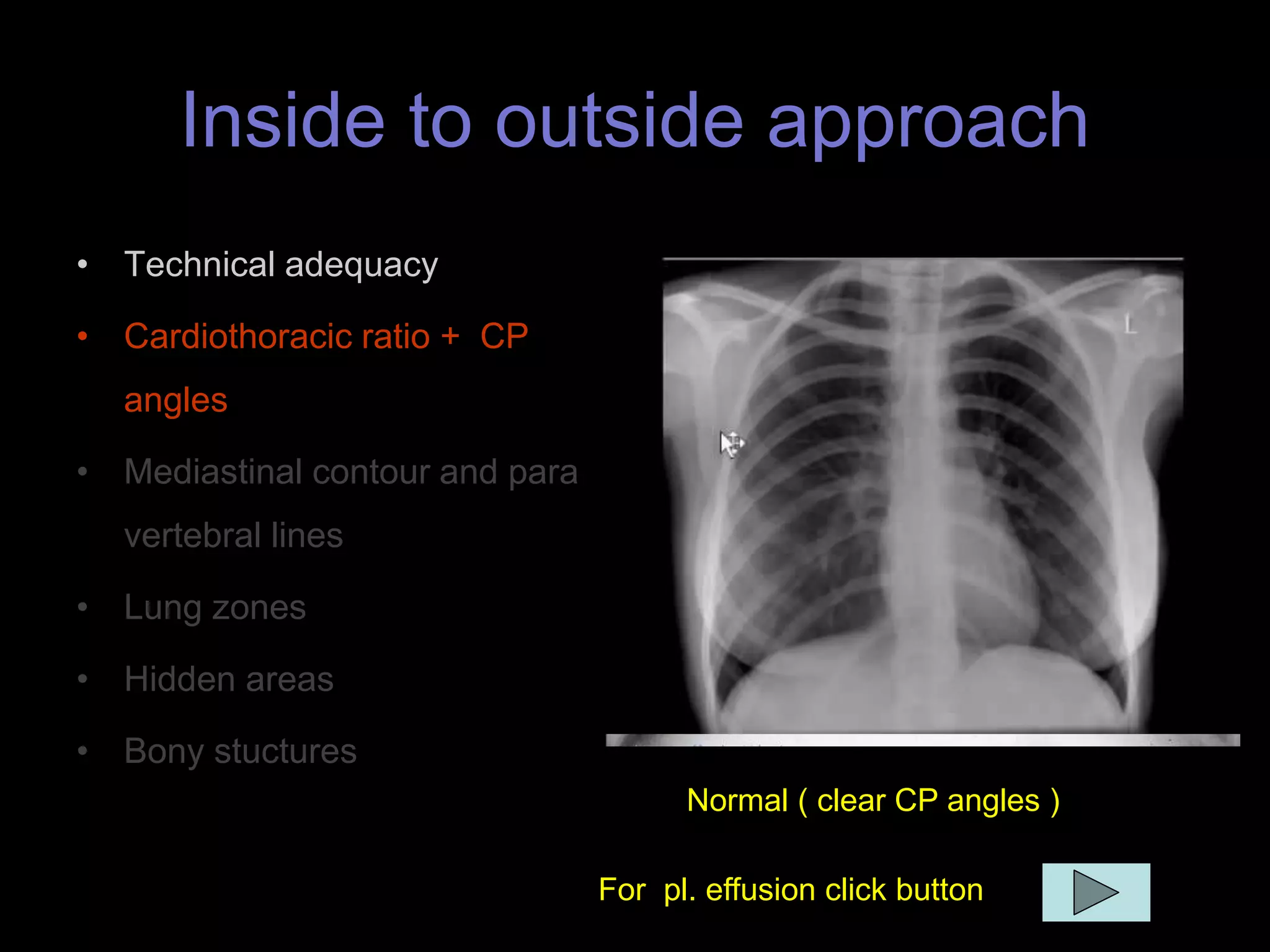
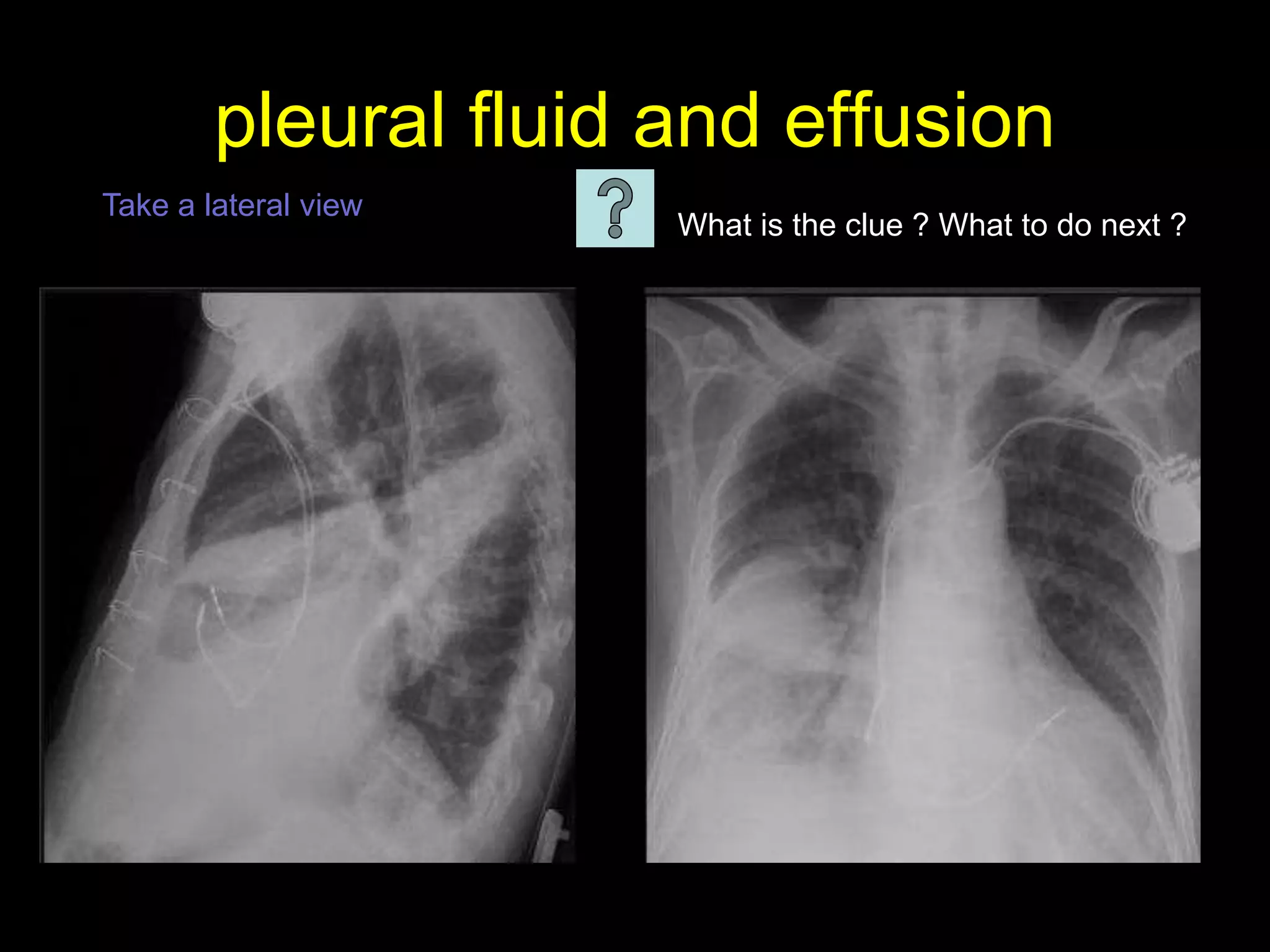
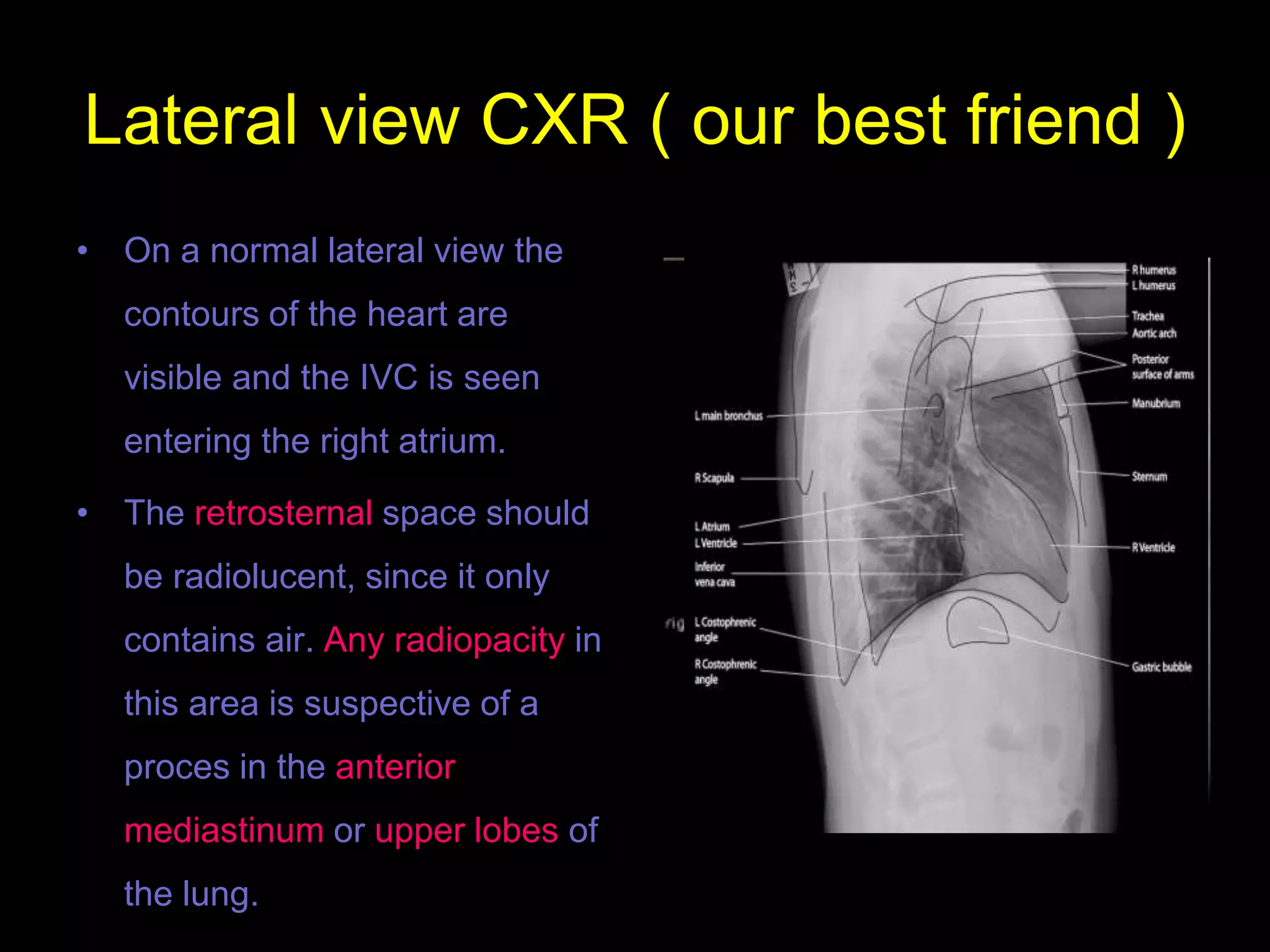
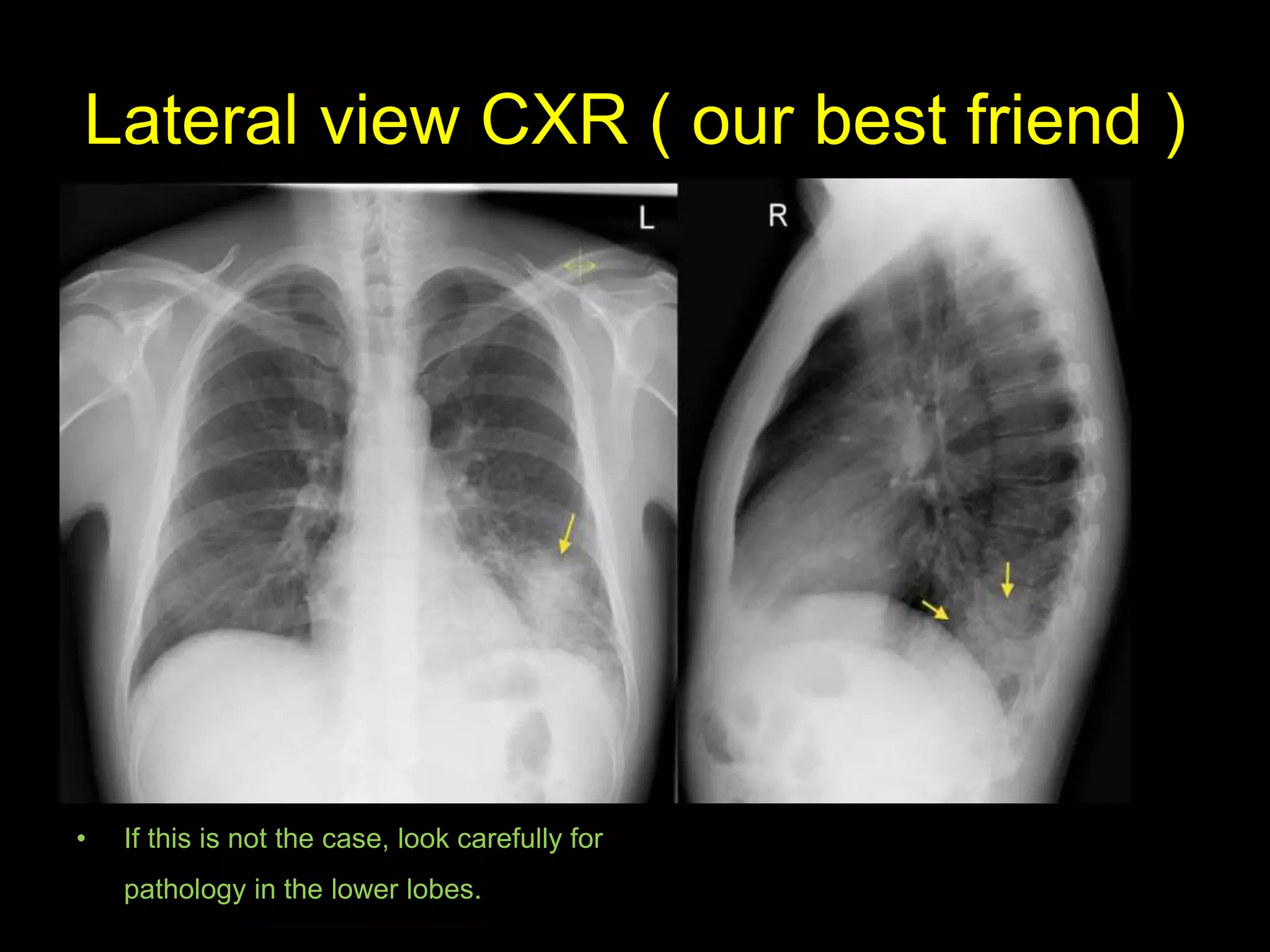
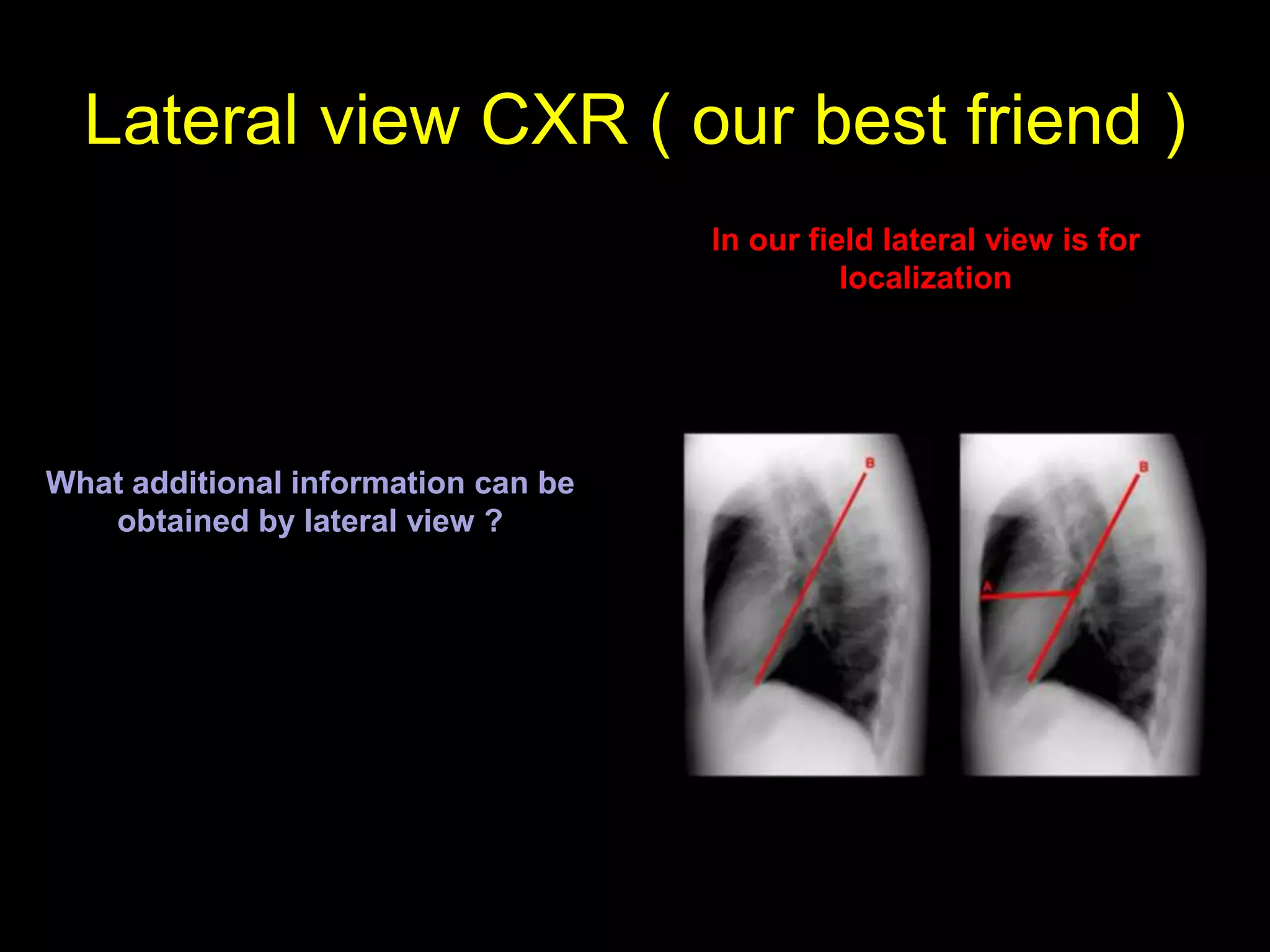
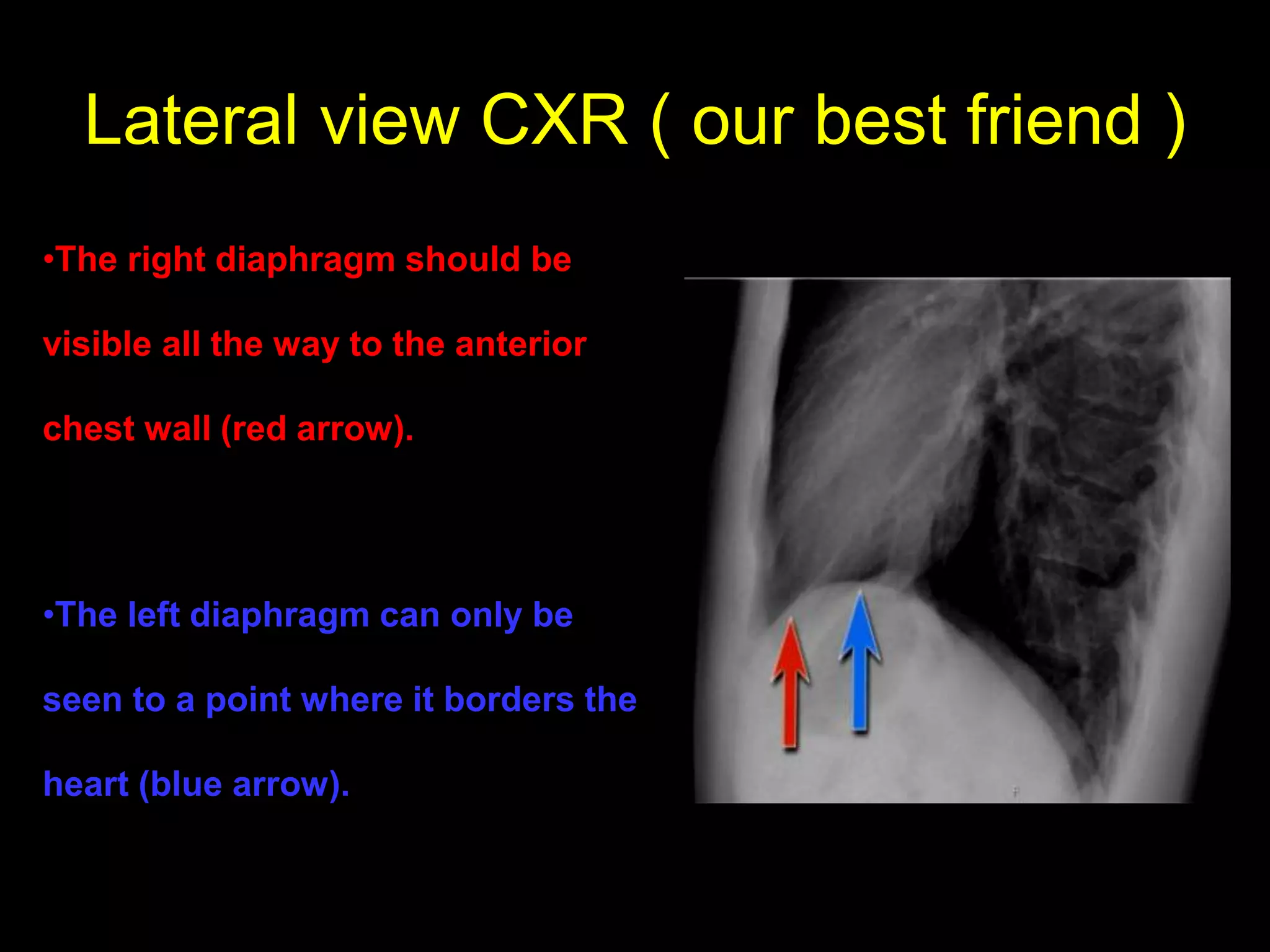
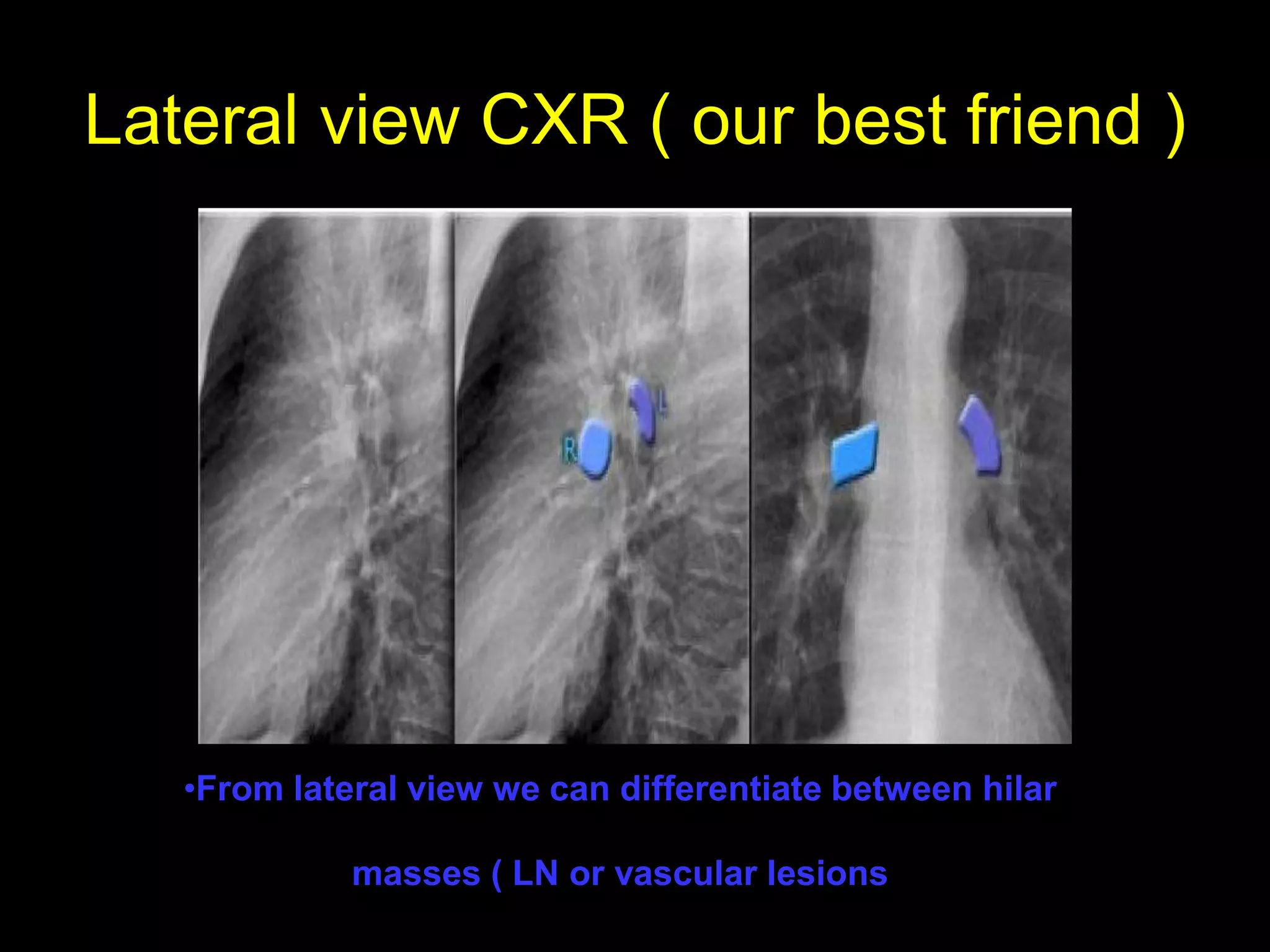
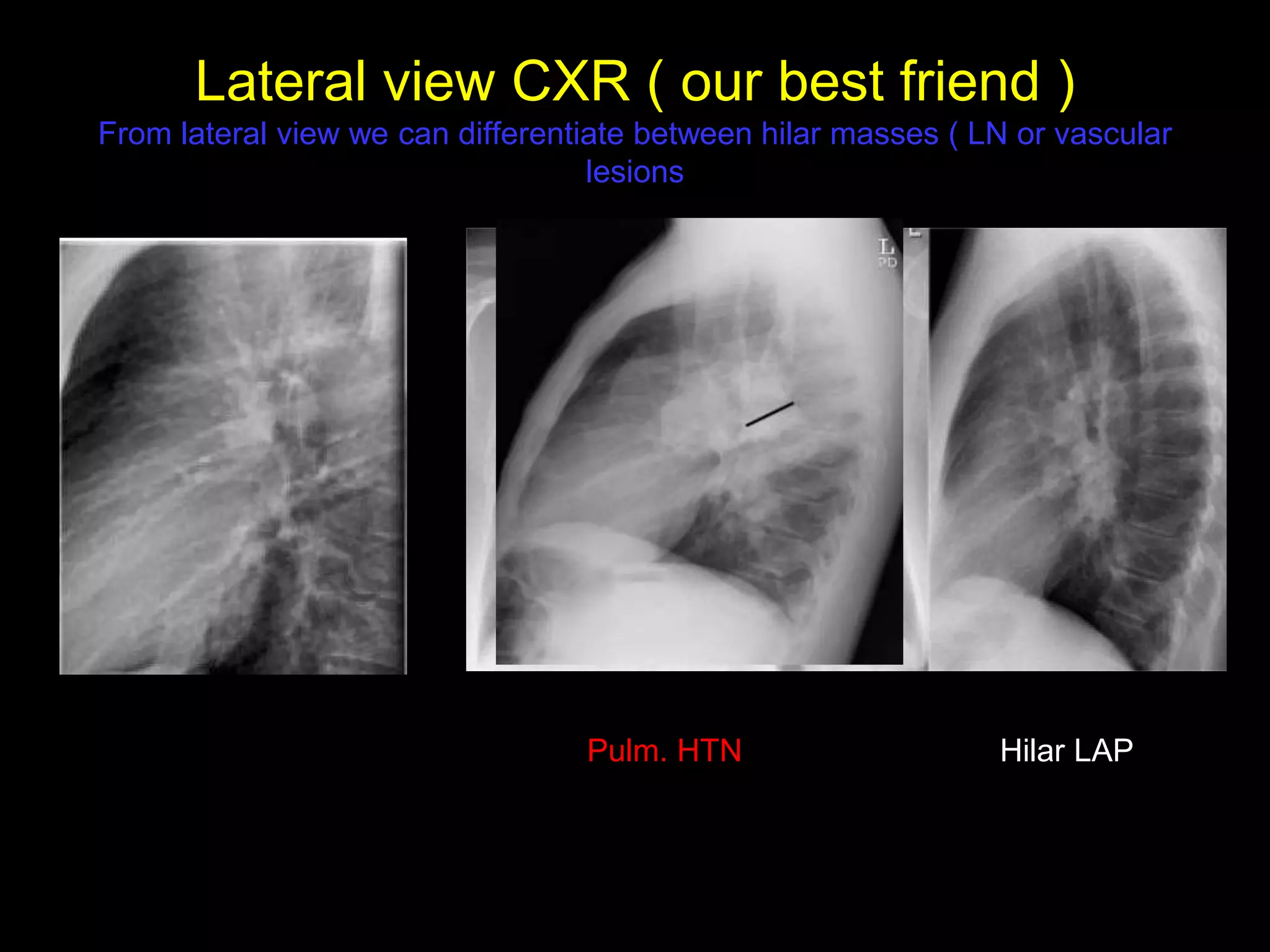
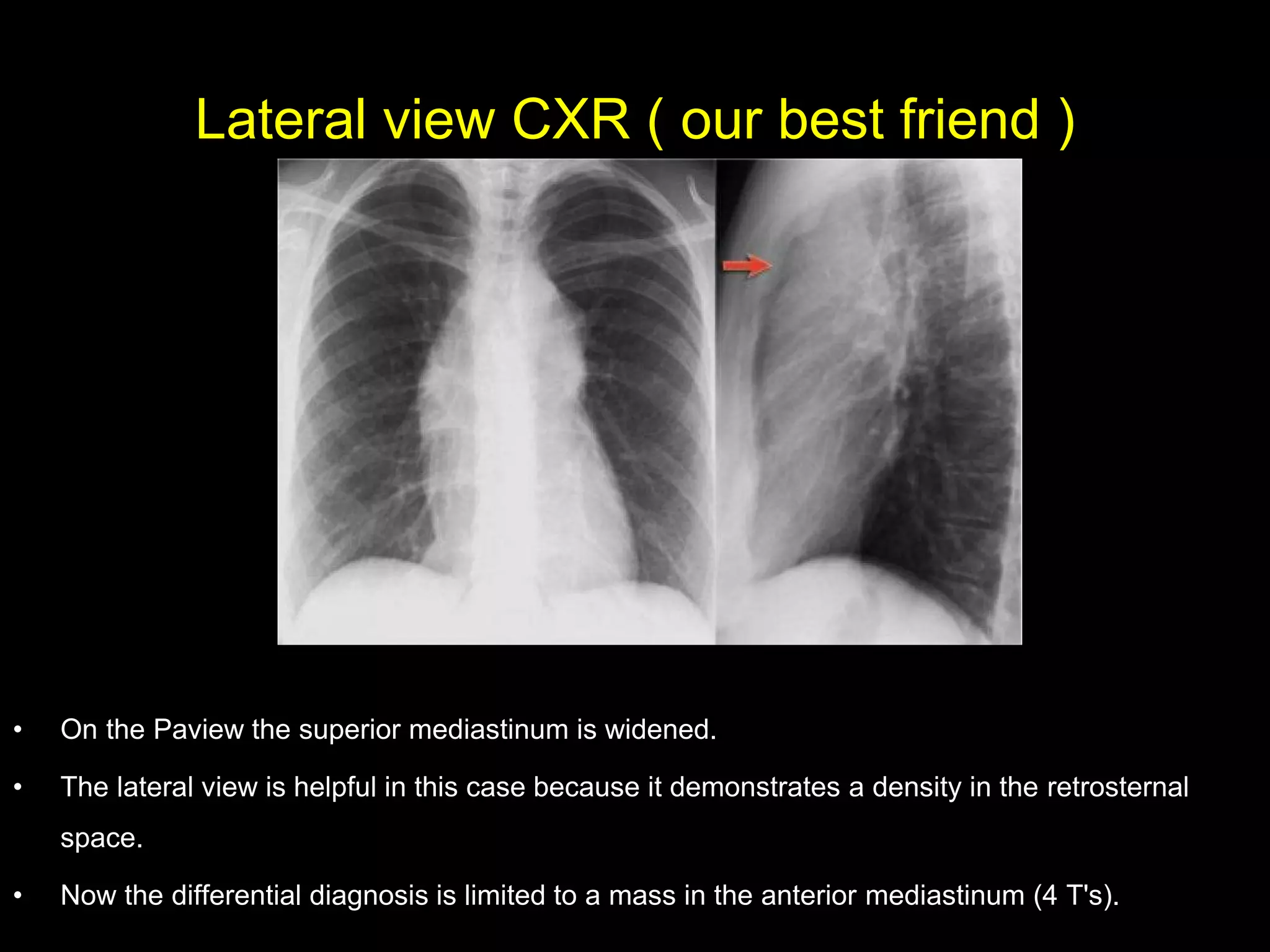
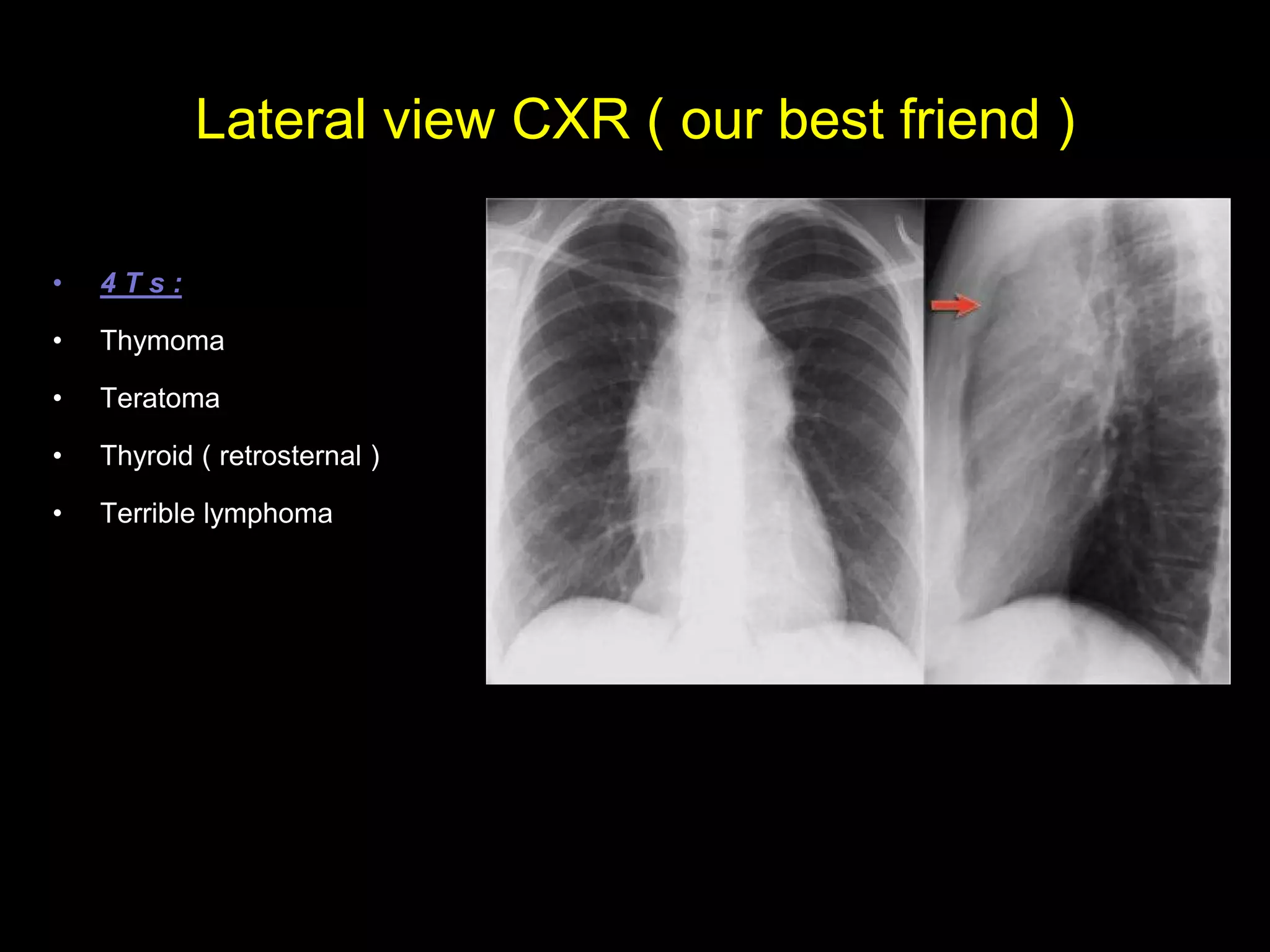

This document provides an overview of the basic approach to interpreting chest X-rays. It discusses evaluating technical adequacy, the cardiothoracic ratio, mediastinal contours, lung zones, and bony structures. Common normal variants like the azygos lobe fissure are also addressed. The lateral view is described as helpful for localization of abnormalities and differentiating hilar masses. Key areas like pleural effusions, diaphragm abnormalities, and the anterior mediastinum are highlighted. An inside-to-outside approach is suggested starting with technical adequacy and moving outward.










































![Radiological_diagnosis_of_TB_ECHO_MOH[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicaldiagnosisoftbechomoh1-240905083452-eb26e5f9-thumbnail.jpg?width=640&height=640&fit=bounds)







































