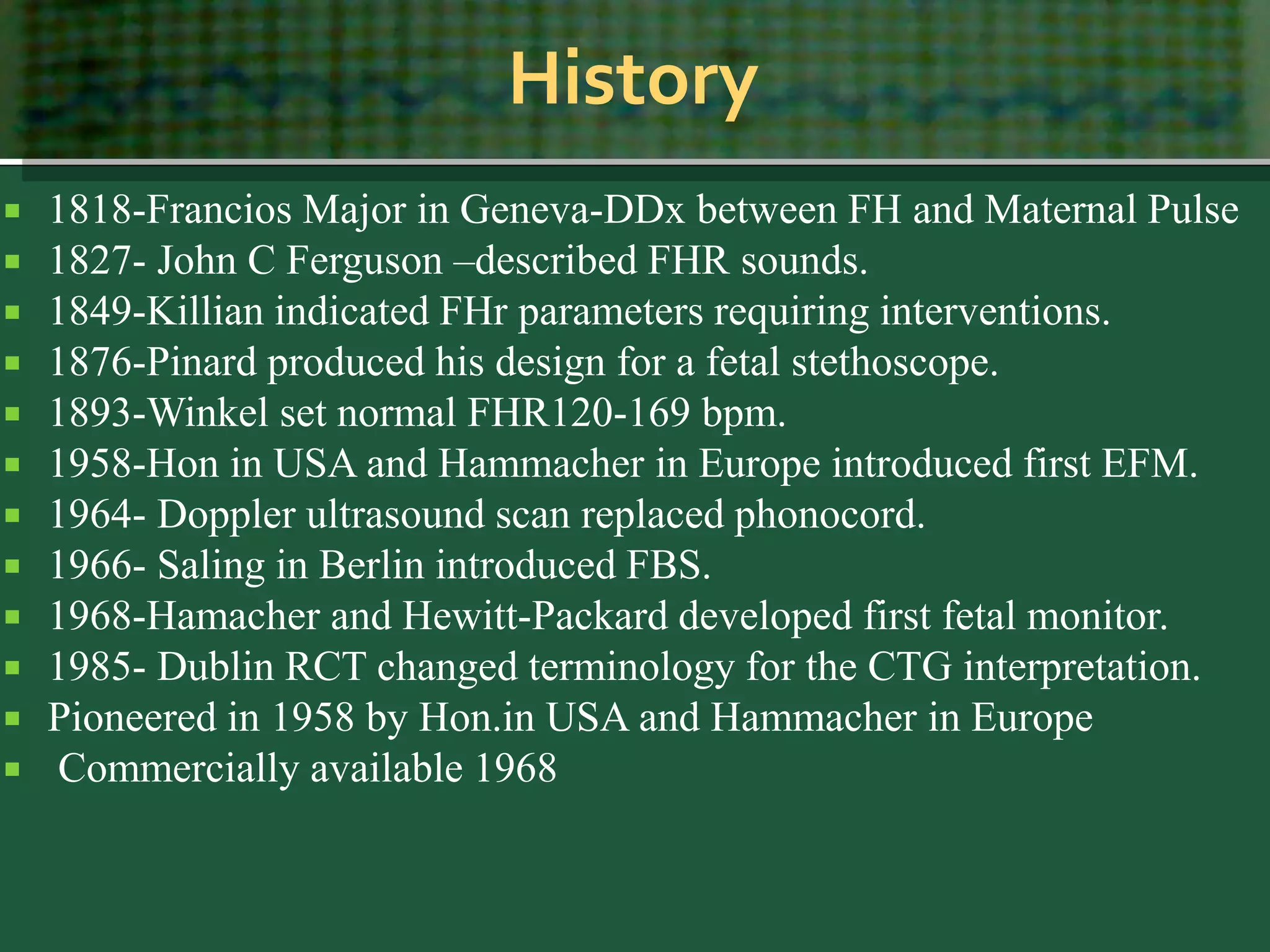
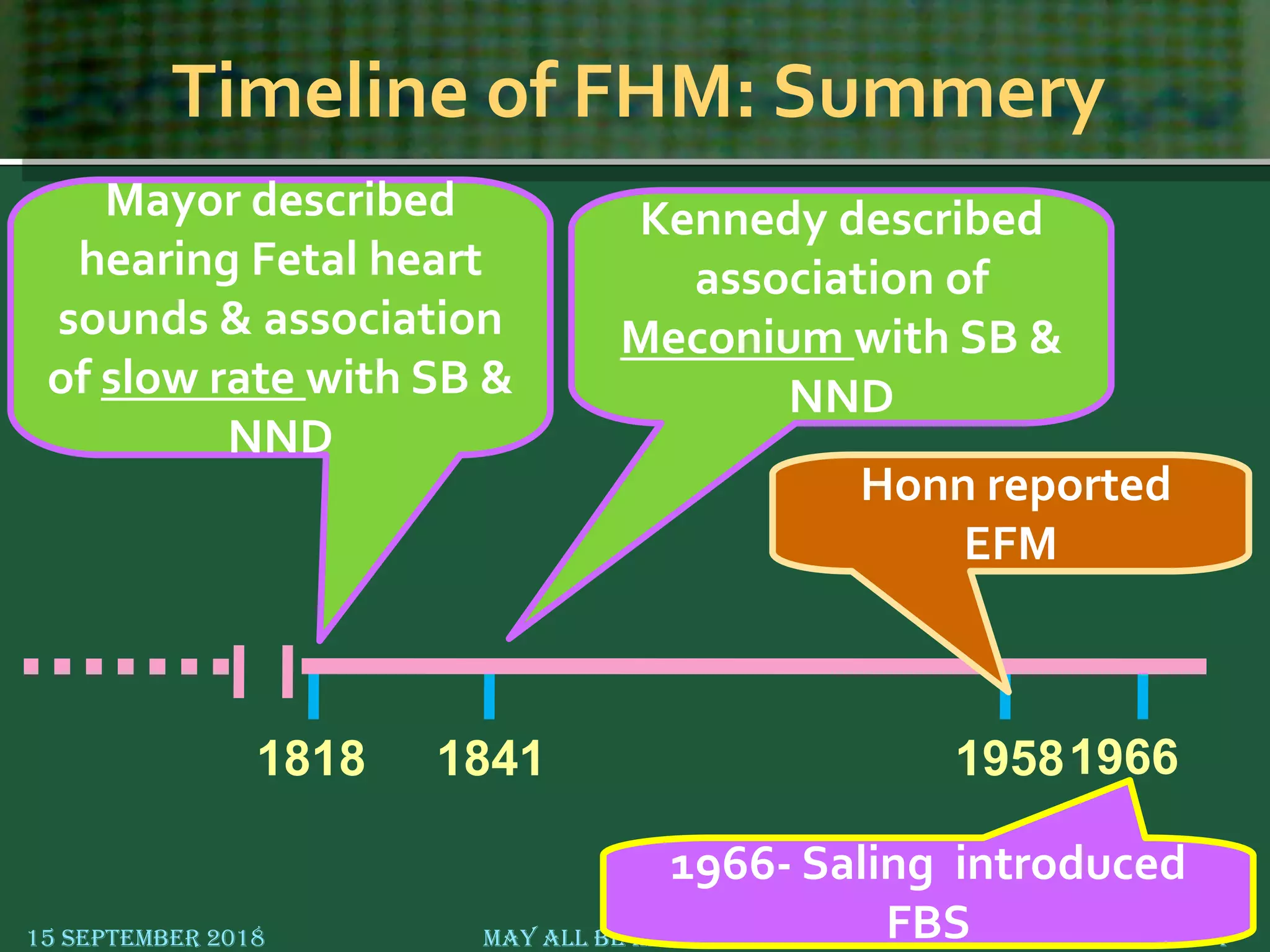
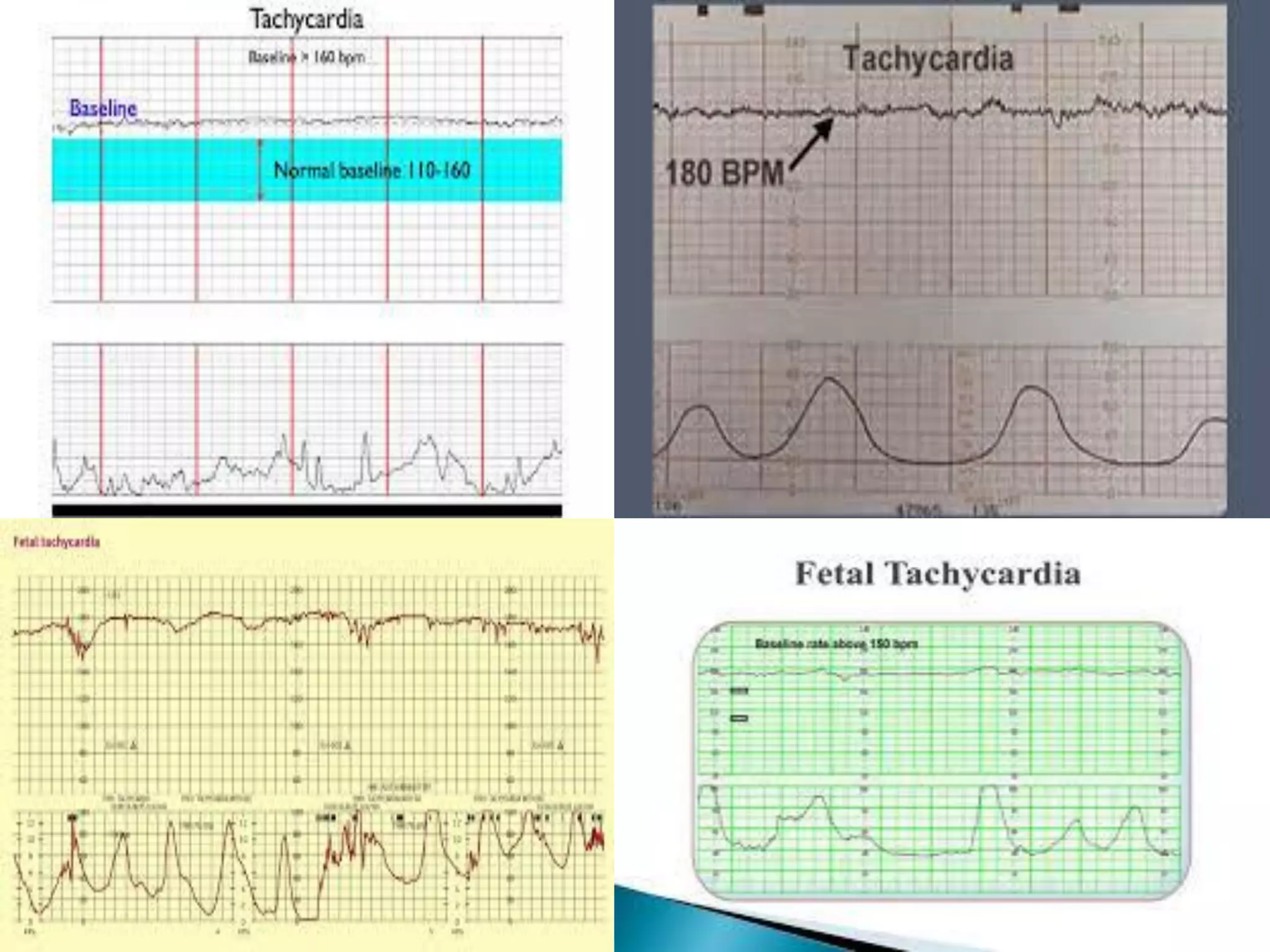
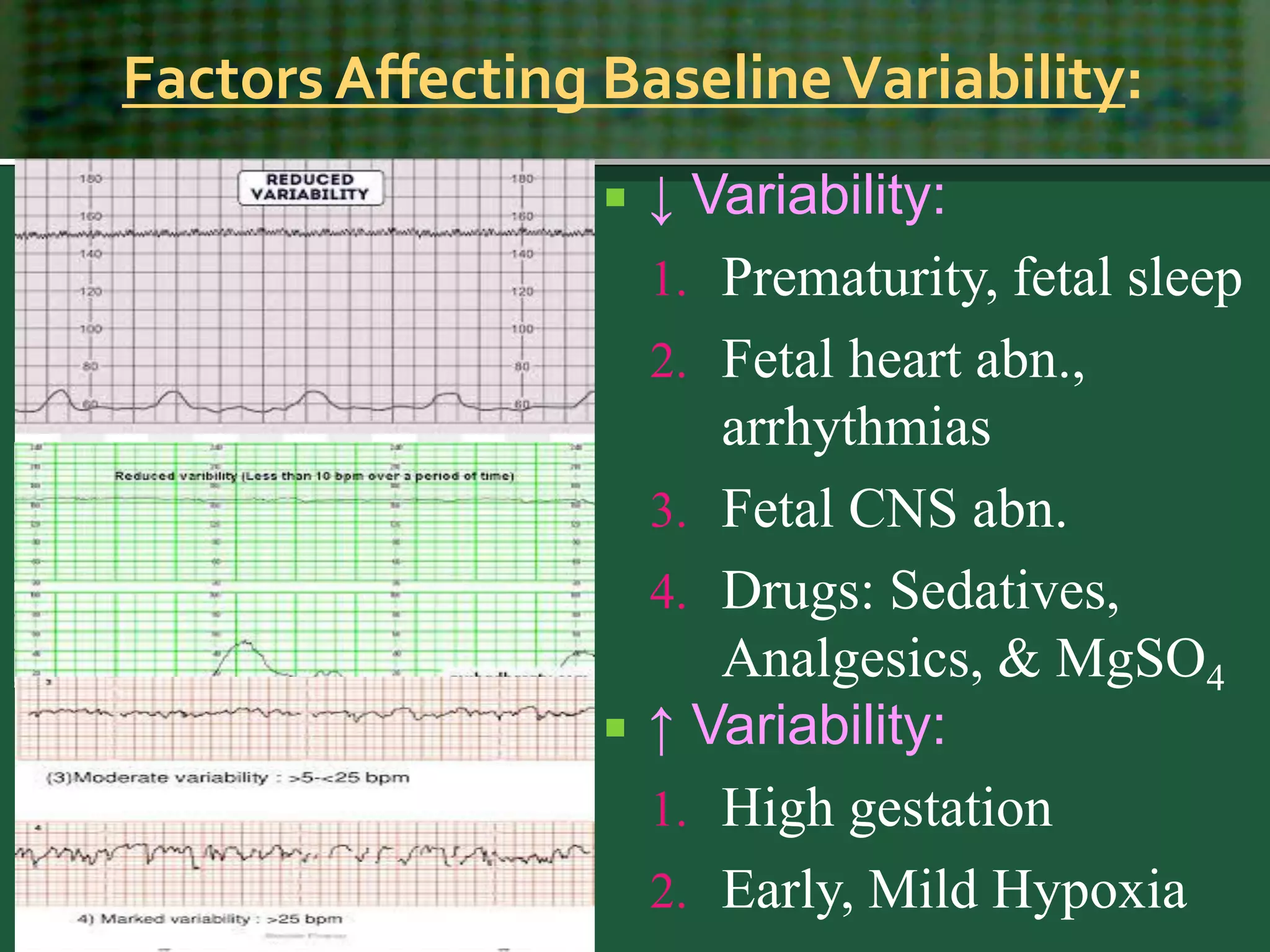
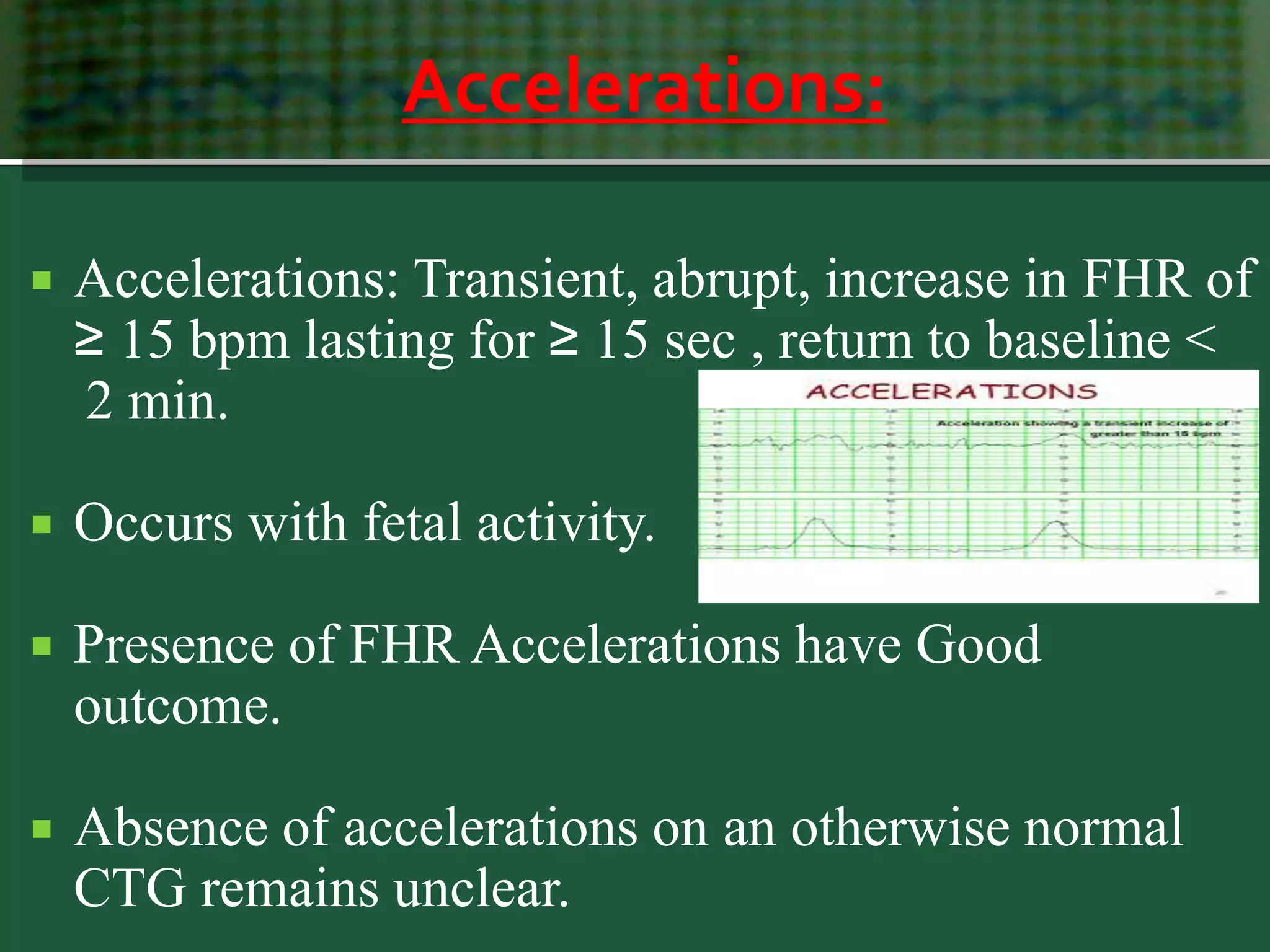
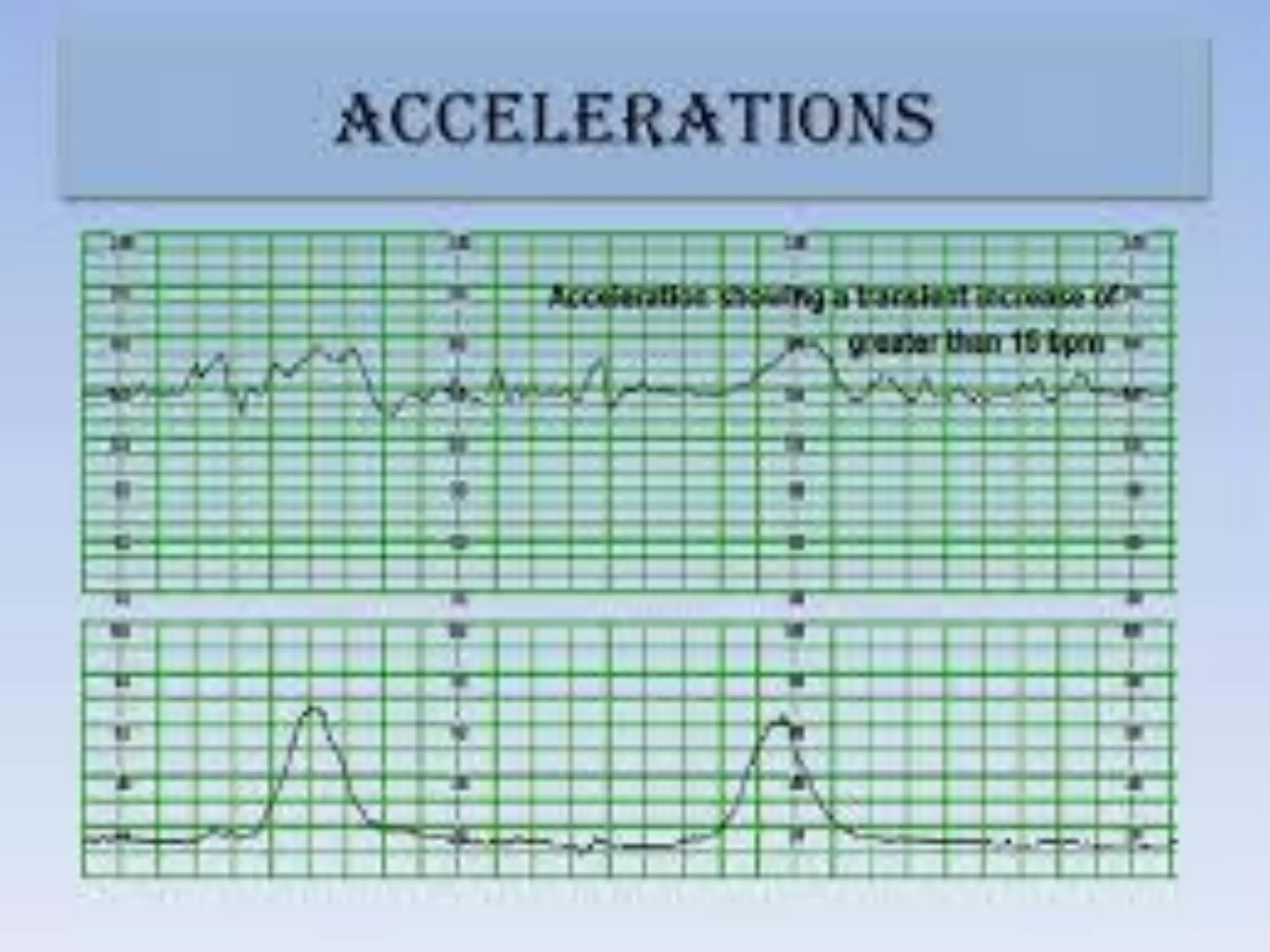
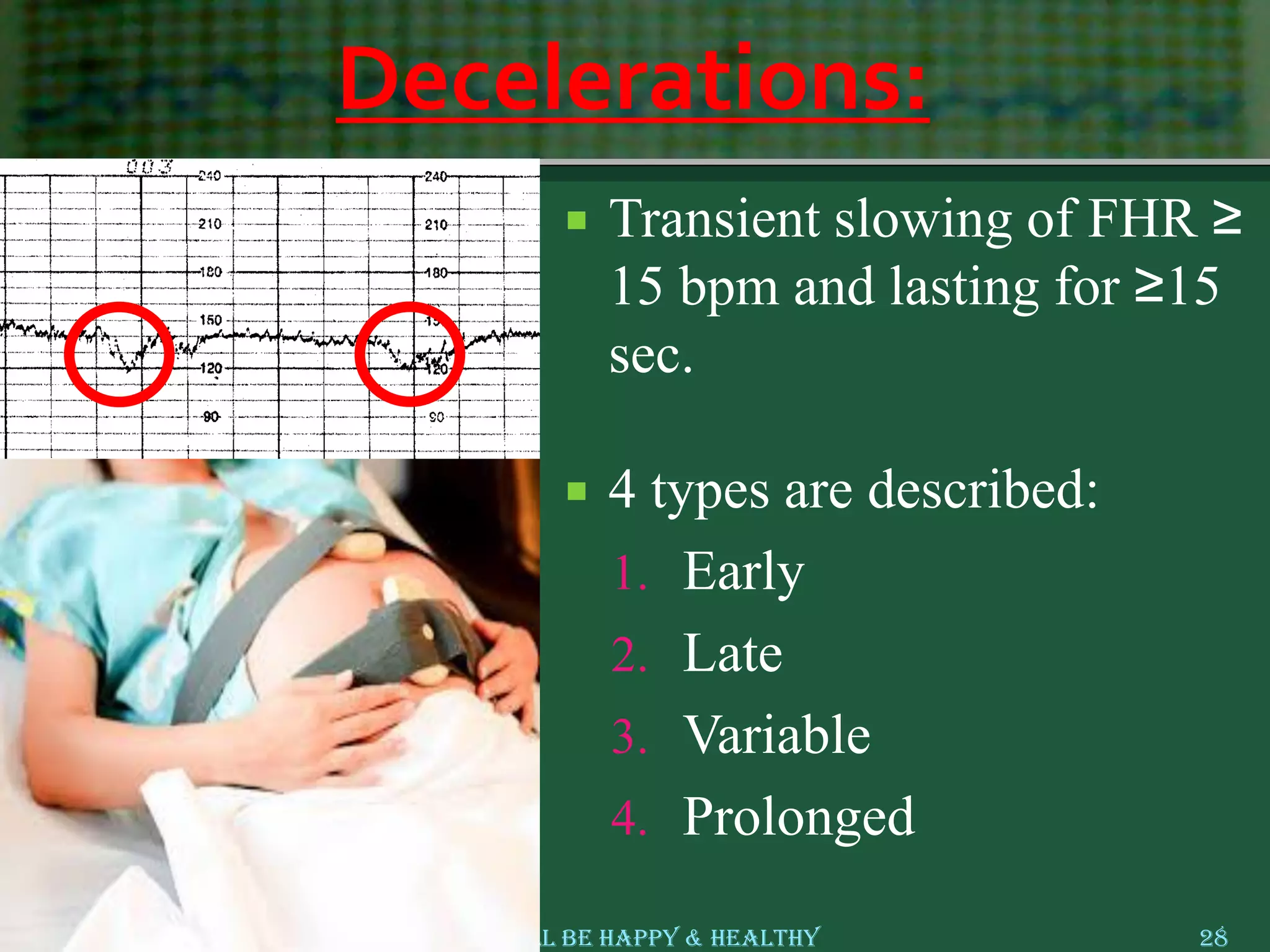
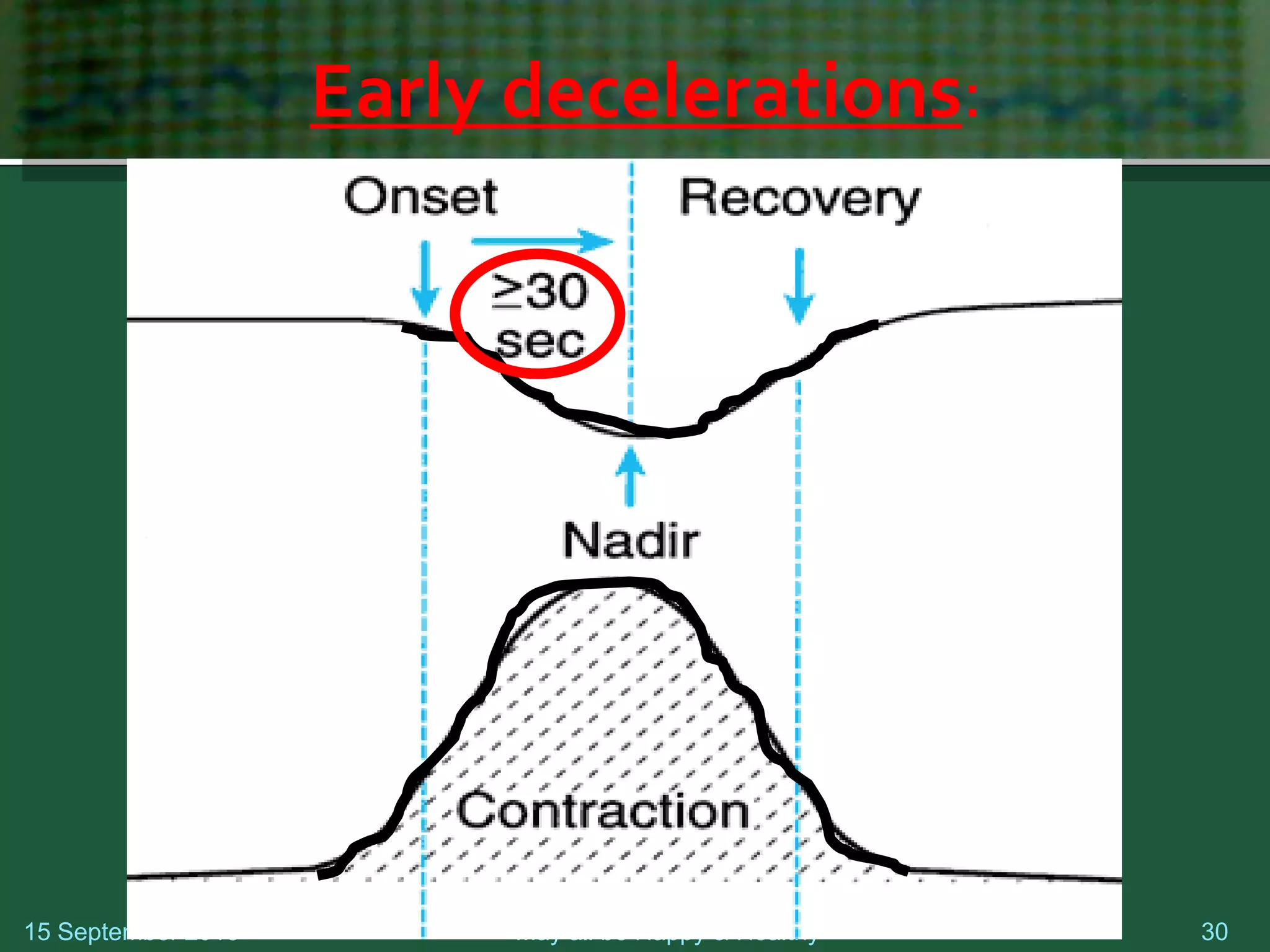
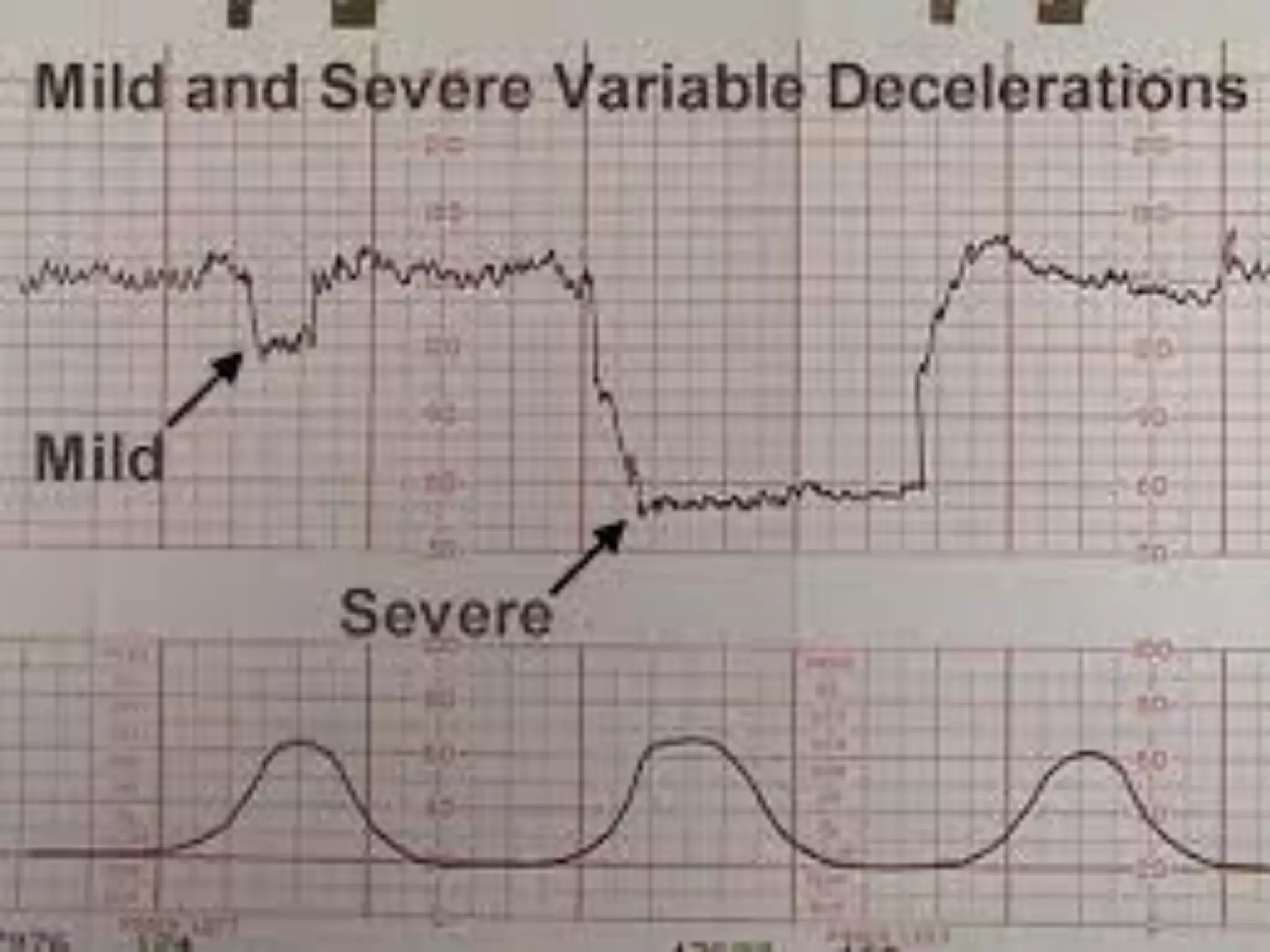
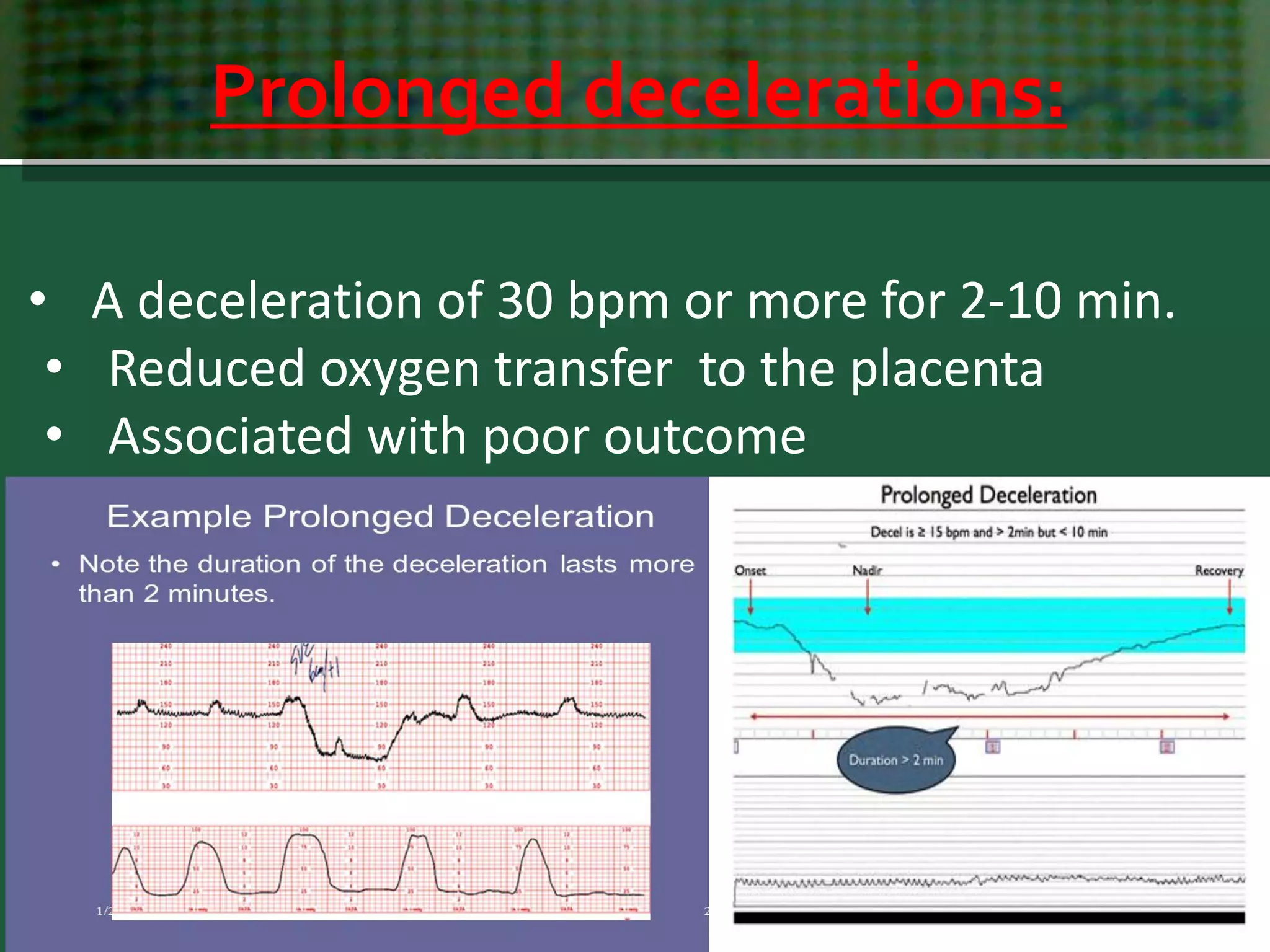
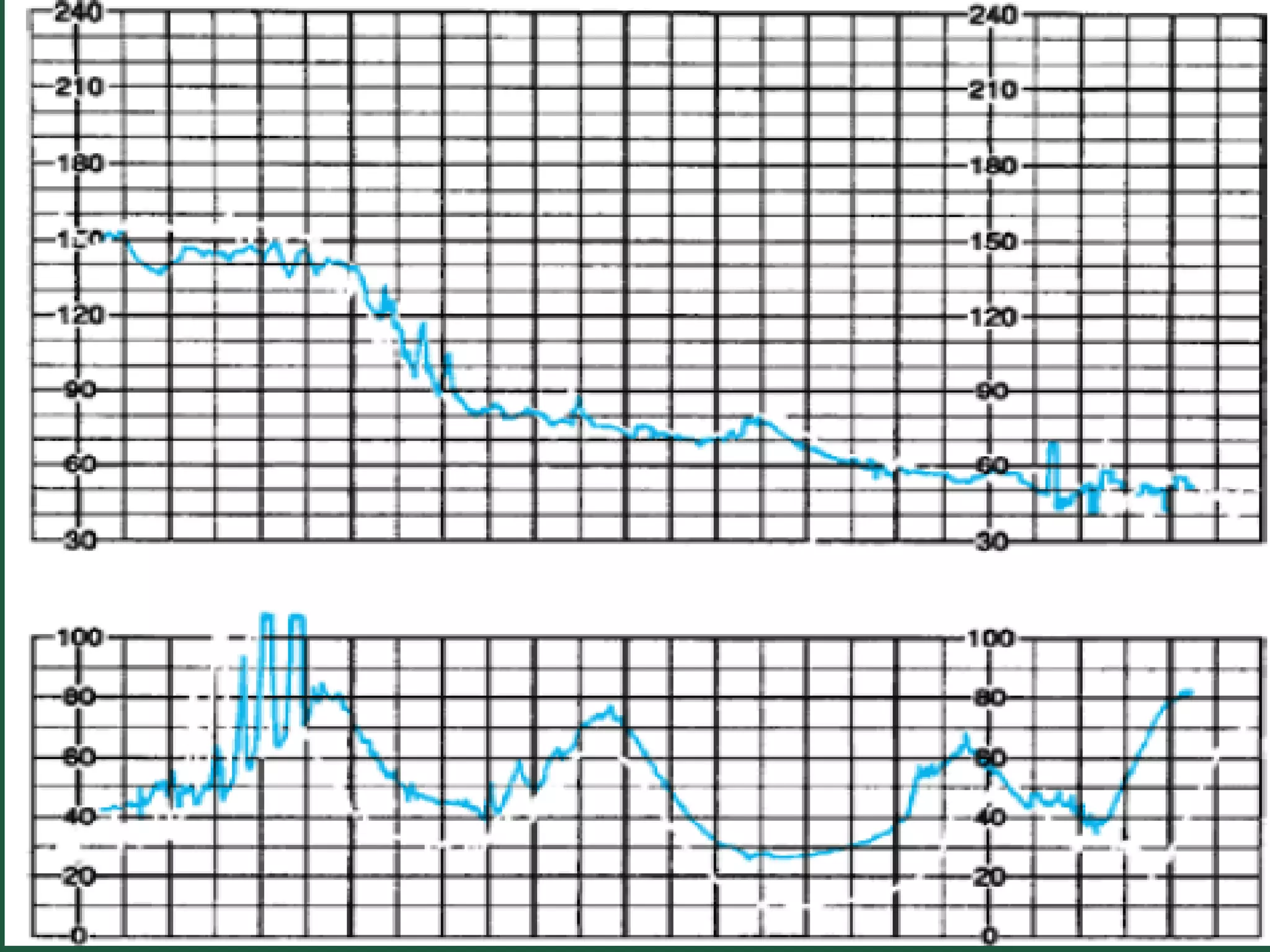
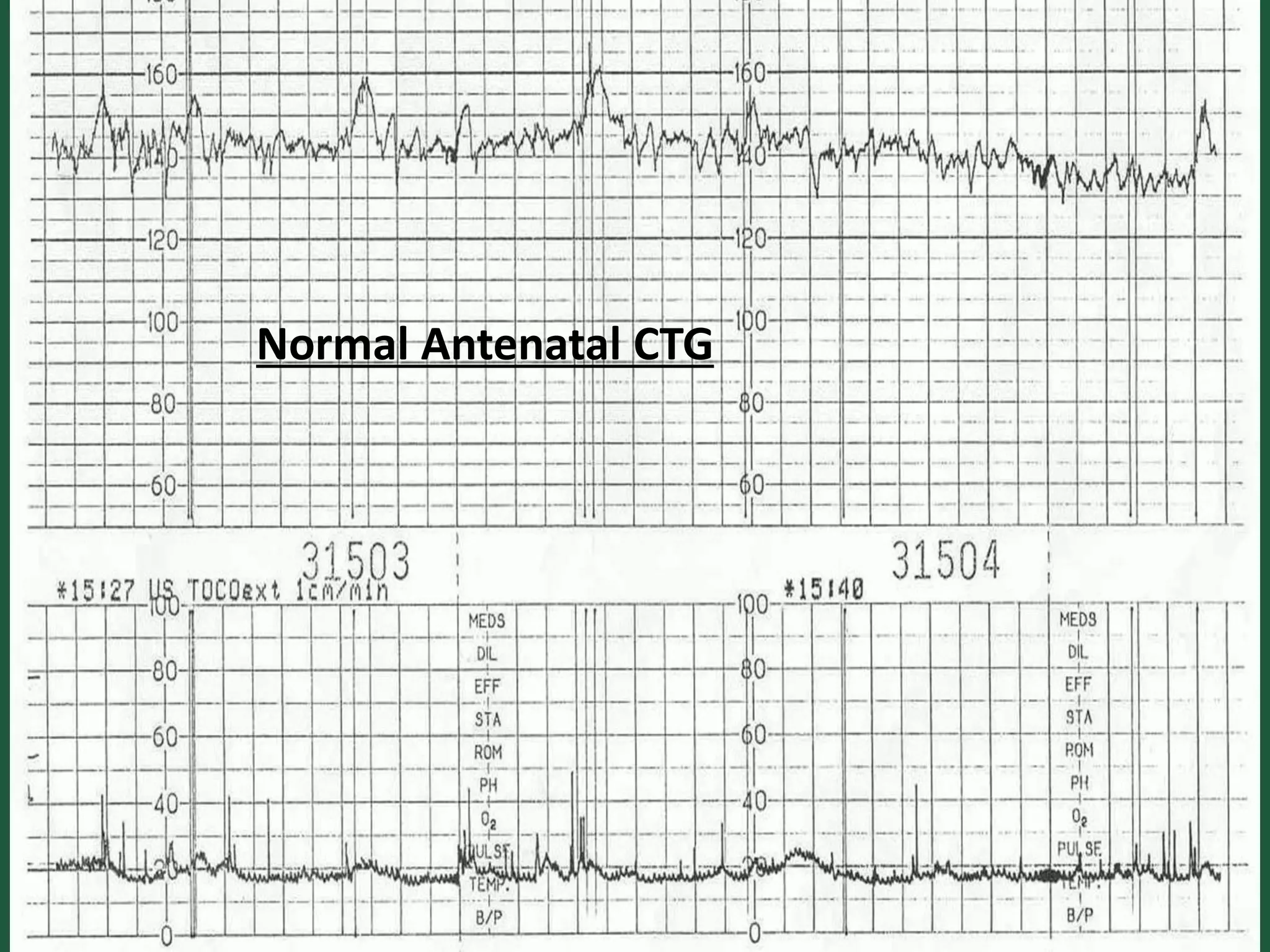
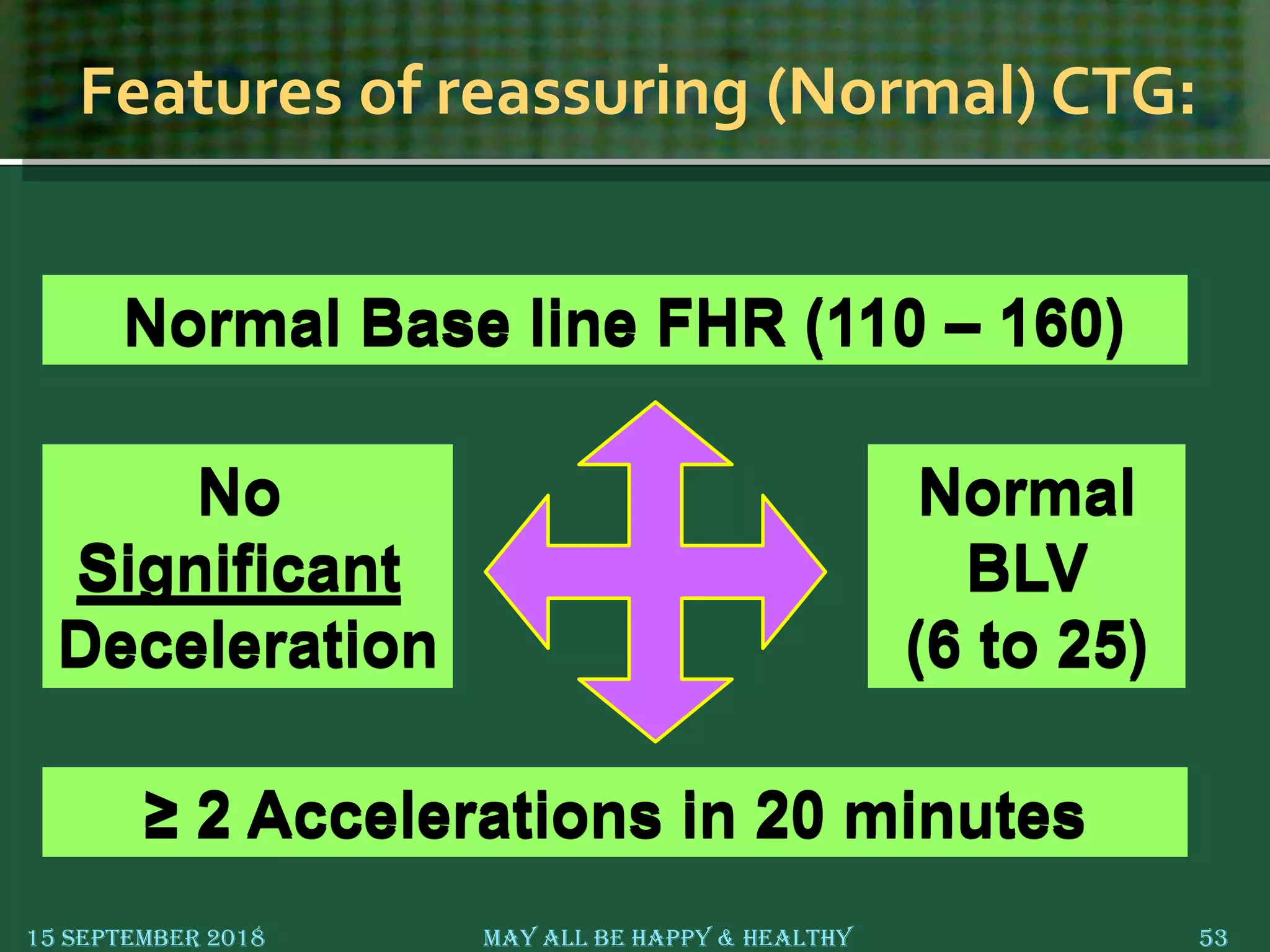
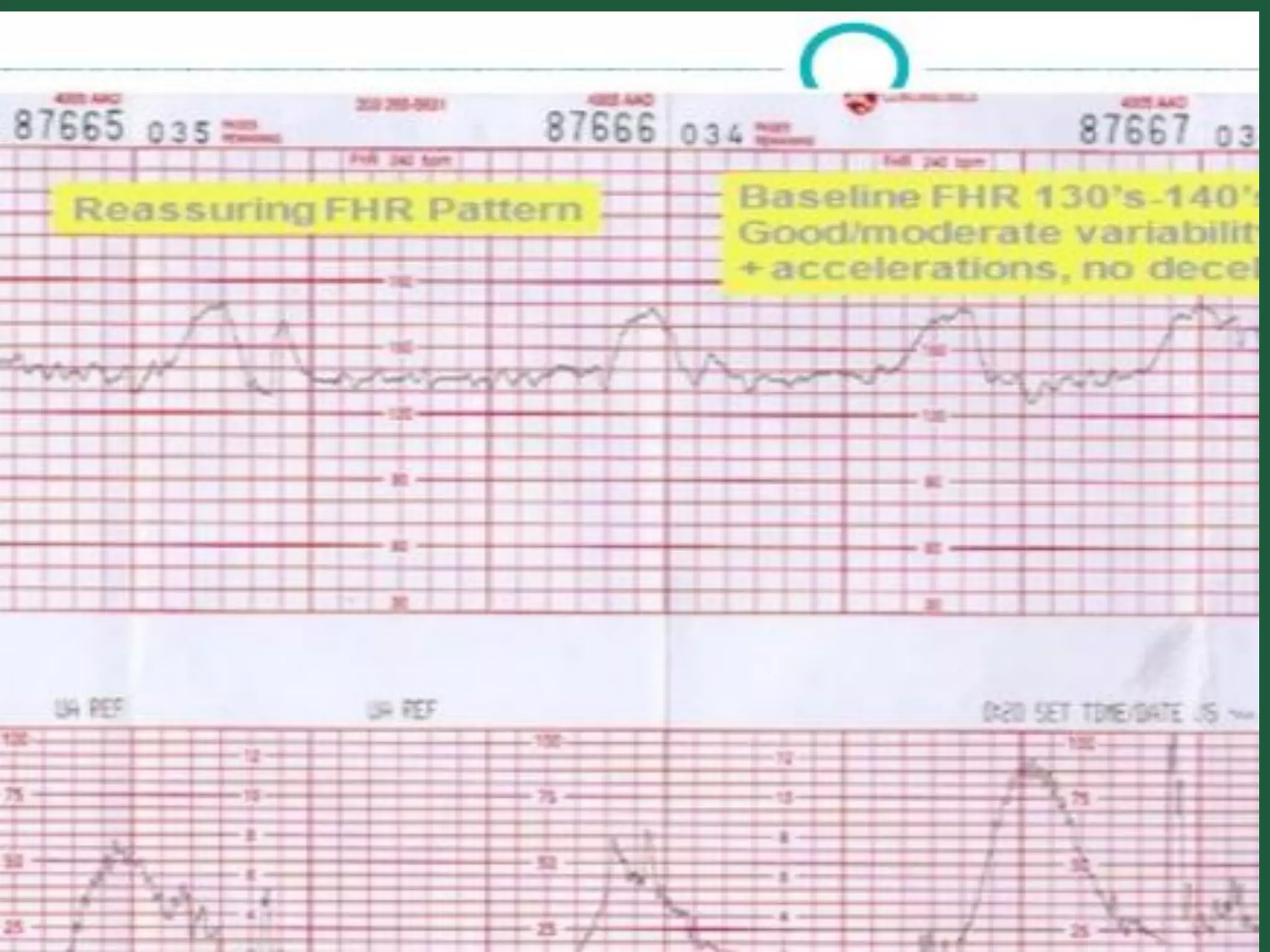
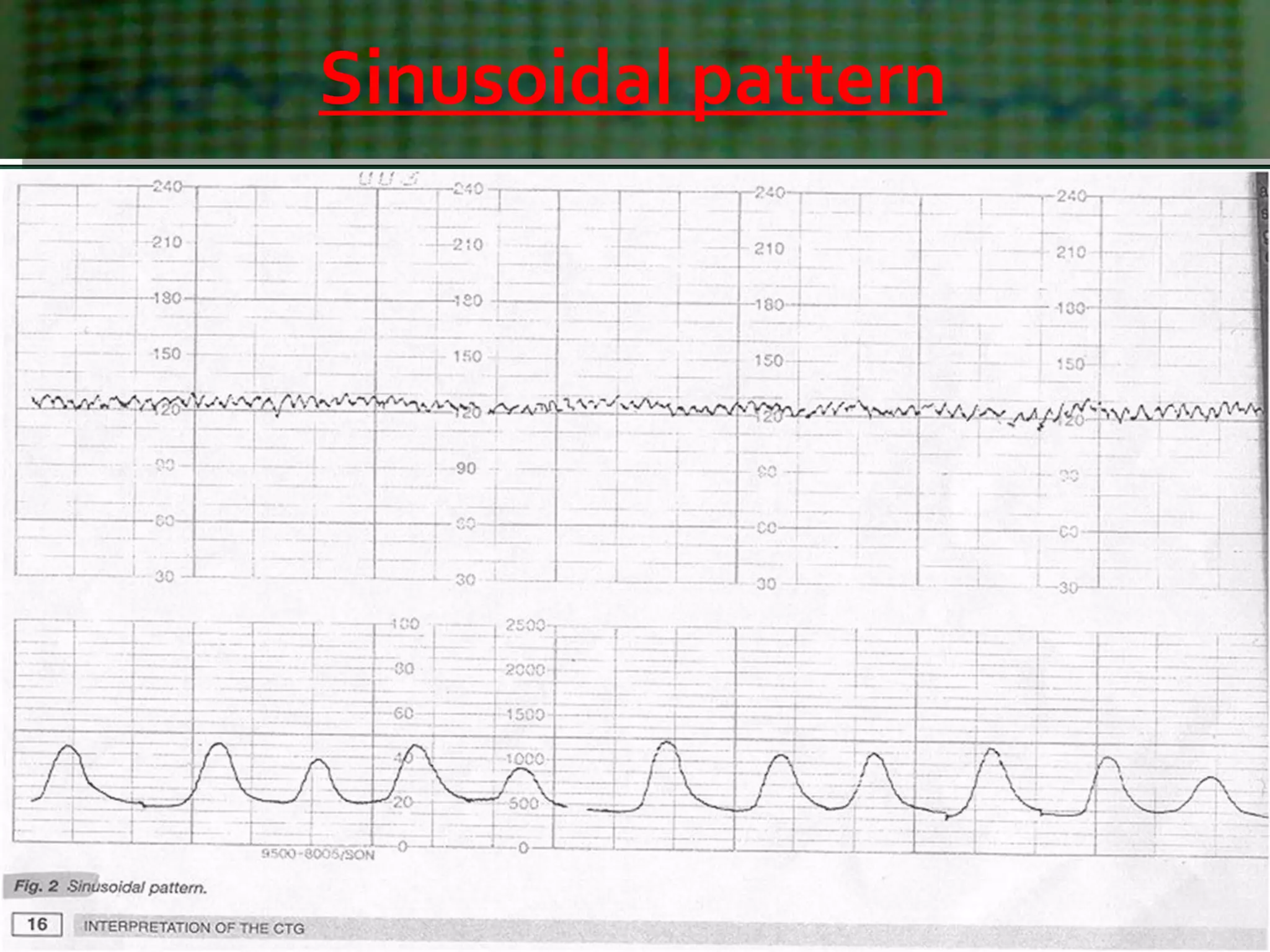
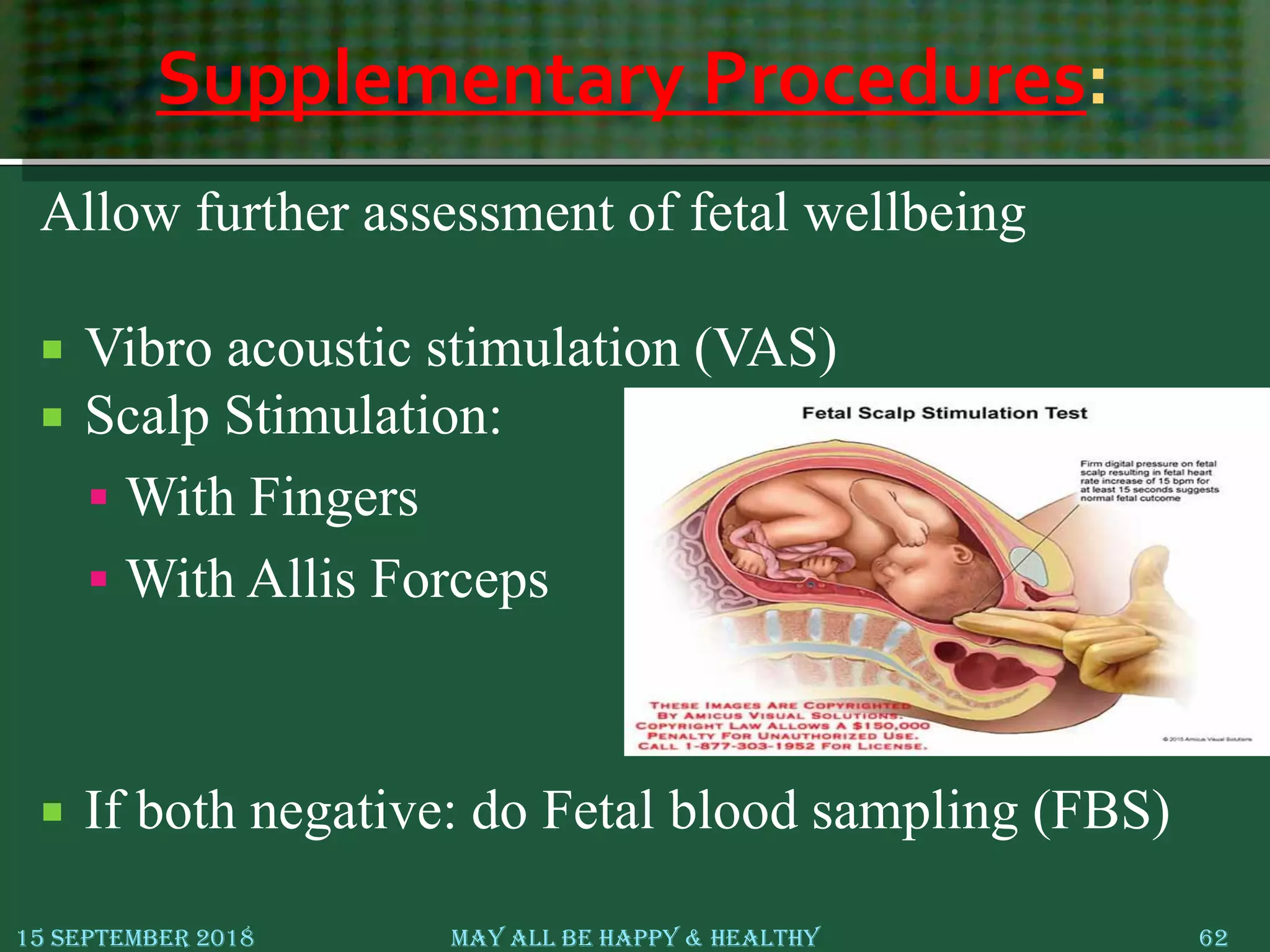
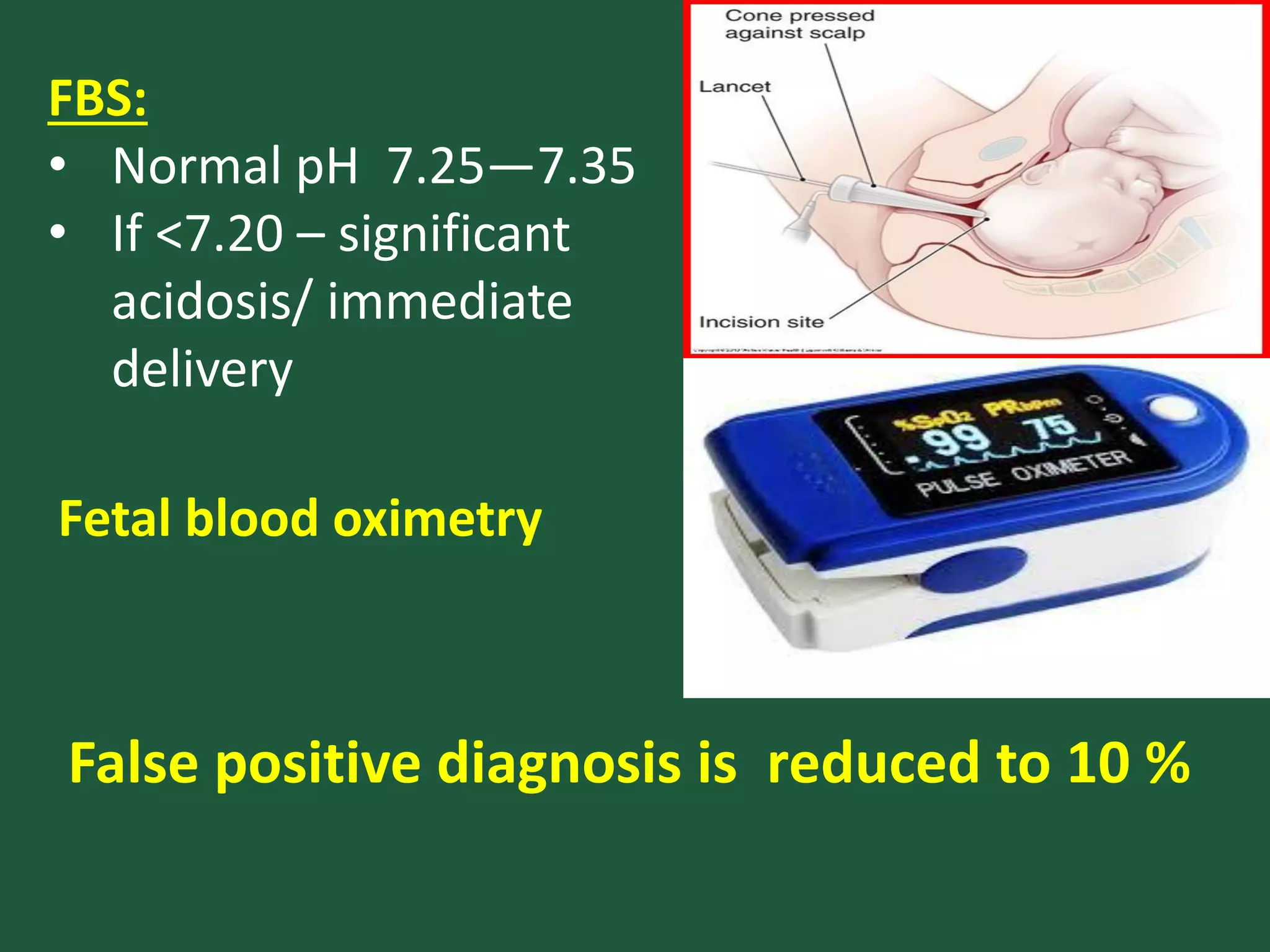
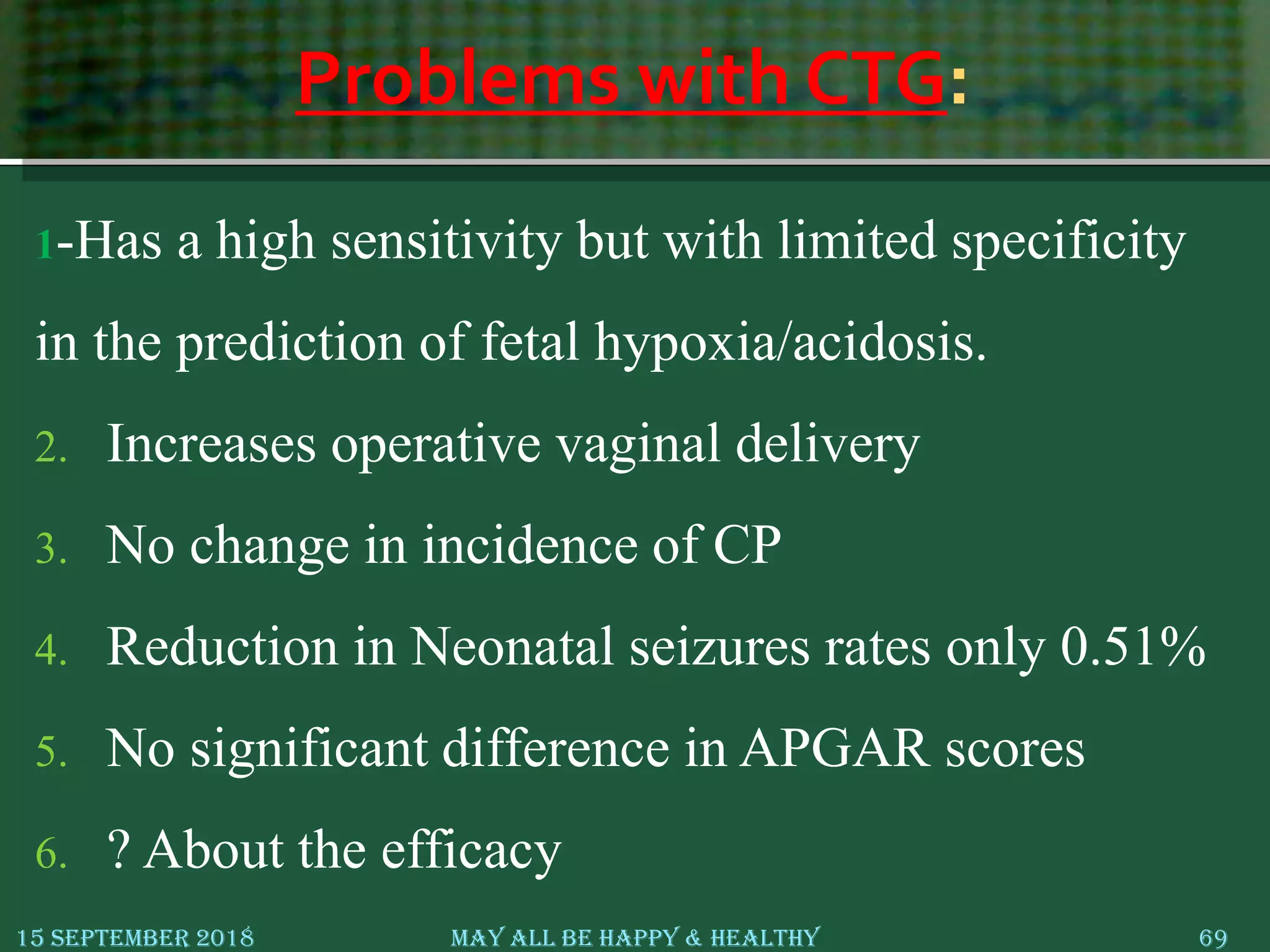
This document provides an overview of cardiotocography (CTG), which is the continuous monitoring of fetal heart rate and uterine contractions during pregnancy and labor. It discusses the history of CTG, indications for monitoring, CTG parameters including baseline heart rate, variability, accelerations, and decelerations. The different types of decelerations like early, late, variable and prolonged are defined. Interpretation of normal versus non-reassuring CTG tracings and management of non-reassuring tracings is covered. Supplementary procedures like fetal blood sampling that can further assess fetal wellbeing are also summarized.