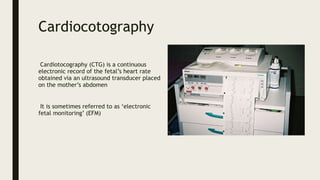
Cardiotocography (CTG) is a technique that uses ultrasound to monitor the heart rate of the fetus and the contractions of the uterus during pregnancy and labor. It allows doctors to monitor the fetal heart rate patterns for signs of distress. The key things monitored are the baseline heart rate, variability, accelerations, and decelerations in relation to contractions. Different patterns can indicate issues like hypoxia. Continuous monitoring is recommended for high-risk pregnancies or when oxytocin is used during labor due to increased risk of complications. CTG provides important information to assess fetal wellbeing during delivery.