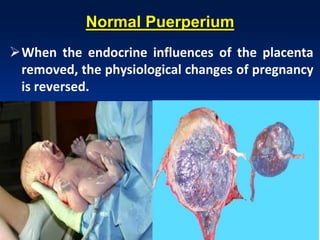
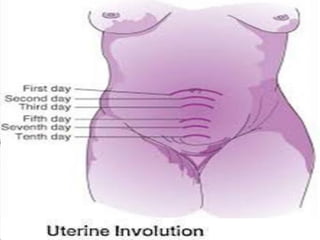
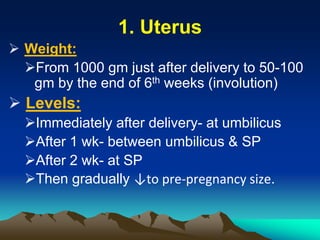
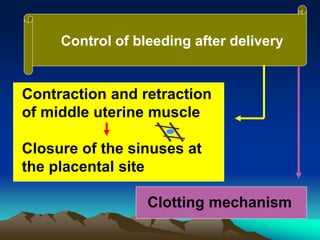
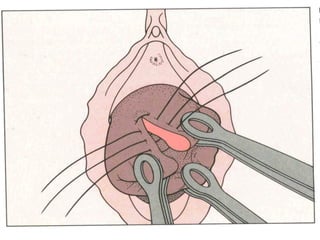
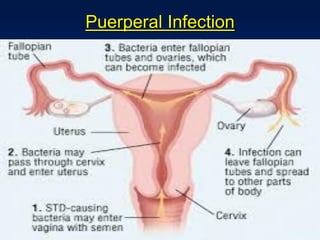
This document discusses normal puerperium and some abnormalities that can occur. The postpartum period is divided into three stages: immediate (first 24 hours), early (first week), and remote (up to 6 weeks). Physiological changes that occur include uterine involution and return of other systems like temperature and blood pressure to pre-pregnancy levels. Potential abnormalities covered include postpartum hemorrhage, puerperal pyrexia (infection), painful perineum, and psychological disorders. Causes, signs, and management are described for these complications.























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









