Downloaded 435 times


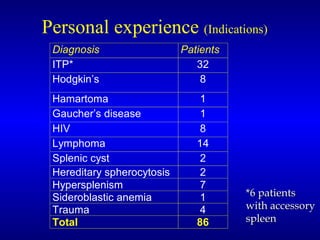
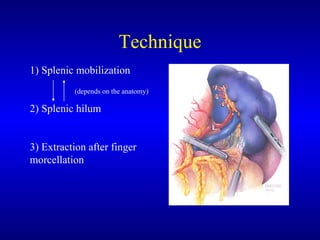
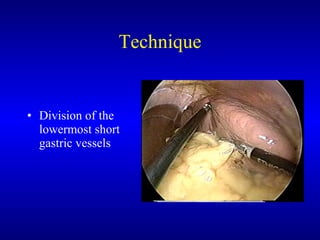
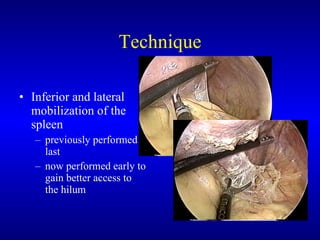

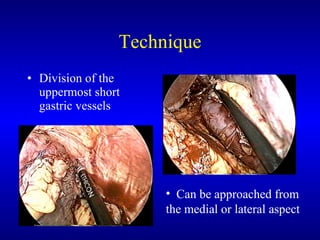

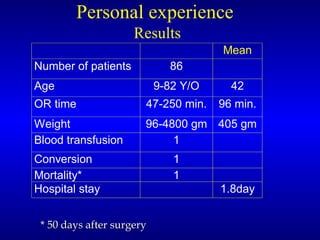


This document discusses laparoscopic splenectomy, including: 1) A brief history of splenectomy and the transition to the laparoscopic approach in the 1990s. 2) Indications for splenectomy including various hematologic disorders, malignancies, and traumatic injuries. 3) Techniques for laparoscopic splenectomy including trocar placement, mobilization of the spleen, and division of hilar vessels. 4) Outcomes data suggesting laparoscopic splenectomy offers benefits over open surgery such as less pain and earlier discharge while having similar operative times.























































































