• The spleenis a large, encapsulated, complex mass of vascular and lymphoid
tissue situated in the upper left quadrant of the abdominal cavity between
the fundus of the stomach and the diaphragm
3.
SPLENECTOMY
• Elective splenectomyis most commonly carried out for idiopathic thrombocytopenic
purpura (ITP) and haemolytic anaemia
• Laparoscopic splenectomy is the standard approach for elective splenectomy ,The
advantages of laparoscopic splenectomy include less postoperative pain, more rapid
recovery and fewer respiratory complications when compared to open splenectomy
• Open splenectomy should be reserved for failure of the laparoscopic technique,
emergency splenectomy for trauma and when the necessary laparoscopic skills or
equipment are not available
5.
PREPARATION
• Vaccinate patients2 weeks prior to surgery to decrease the risk of post-splenectomy sepsis
Immunize against pneumococcal infections and Haemophilus influenza type b (Hib) and
meningococcus group C
• Blood product reservation
6.
LAPAROSCOPIC SPLENECTOMY
• Positionthe patient in a left lateral position. This position facilitates retraction of
the stomach and omentum away from the spleen and improves access
• Create a pneumoperitoneum using a Veress needle technique at the umbilicus or
an open technique at the camera port site
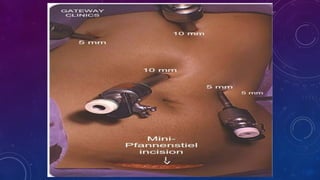
• Exact port placement depends on the size of the spleen. For a normal sized
spleen place the 11-mm camera port above the umbilicus and to the left of the
midline. Place a 5-mm port in the epigastrium and a 12-mm port for stapler and
retrieval bag in the left lateral position .An additional port for a fan retractor may
be necessary.
8.
• Perform asystematic exploration looking for splenunculi (small nodules of
splenic tissue away from the main body of the spleen), which may be found
anywhere in the abdominal cavity, but are commonly located at the hilum of
the spleen and adjacent to the tail of the pancreas
• retract the spleen medially. Divide splenic attachments about 1 cm away from
the spleen and use these attachments to retract the spleen
9.
• Continue thedissection, using the harmonic scalpel or hook diathermy, from the inferior
pole of the spleen to the superior pole and spleen can be moved medially to expose the
back of the splenic hilum .
• Return to the lower pole of the spleen and begin the medial dissection by dividing the
serosa over the hilar vessels
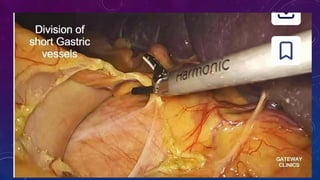
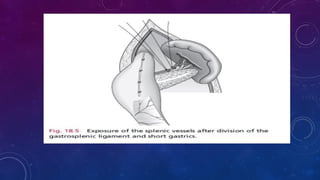
• Pass towards the upper pole of the spleen for short gastric vessels. Divide these with
the harmonic scalpel. Alternatively, they can be divided together with the hilar vessels
using a vascular stapler.
• A fan retractor may be used by the first assistant from the right upper quadrant position
to retract the splenic flexure and, later in the procedure, to retract the stomach away
from the spleen.
11.
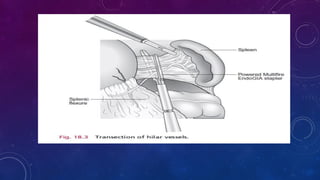
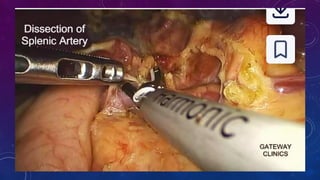
• Once aclear view in front and behind the hilum is obtained, place a vascular
stapler across the vessels at the hilum of the spleen and divide the splenic
artery and vein. Take care to remain close to the spleen as straying medially
may damage the tail of the pancreas.
• Once all the vessels are divided, lift the spleen anteriorly to allow division of
any remaining posterior attachments using a harmonic scalpel
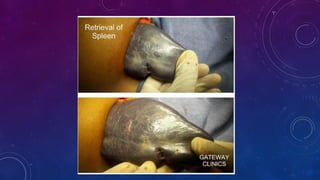
• The splenophrenic ligaments at the top of the spleen to stop it falling into the
abdominal cavity: these are divided once the spleen has been placed in the
retrieval bag
26.
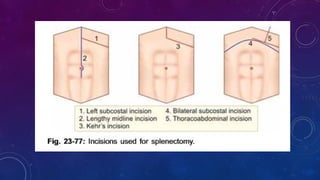
OPEN SPLENECTOMY
• Makean upper midline or left subcostal incision through the abdominal wall
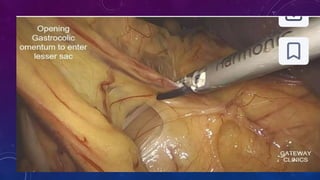
• Ligate the splenic artery at the beginning of the operation if the spleen is very large or
prior to infusing platelets in patients with ITP . the lesser sac entered by dividing 10 cm of
the gastrocolic omentum using diathermy or a harmonic scalpel. Incise the peritoneum at
the superior border of the pancreas to identify the tortuous splenic artery. Use a right
angle forceps to pass a ligature behind the splenic artery and ligate it in continuity with a
large non-absorbable suture
30.
• Dividing lateralattachment lmove the spleen medially and upwards into the
abdominal wound and divide the adhesions from the upper pole of the spleen to
the diaphragm
• Divide the peritoneum over the front of the splenic hilum from the lower pole to
the upper pole. The short gastric arteries are divided
• Divide the splenic vessels with large clips.
31.
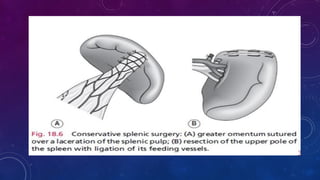
CONSERVATIVE SPLENECTOMY
• Immediatelyremove a spleen that is either fragmented or avulsed from its vascular
pedicle. Under these circumstances consider auto transplantation of splenic tissue by
suturing a piece of omentum around a sliver of removed splenic pulp to encourage
splenic regeneration(splenosis)
• If the extent of the damage and bleeding is less severe, gently mobilize the spleen
into the wound after dividing its peritoneal attachments. Remove attached clot and
examine the organ thoroughly. Decide whether topical haemostatic agents, partial
splenectomy or some form of splenic repair is feasible, with or without ligation of the
splenic artery or its branches
32.
• Capsular tearsand other minor injuries can often be controlled by
application of a haemostatic agent
• Deeper or more extensive lacerations may still be suitable for repair.
Mobilize the spleen, at least in part. Use synthetic absorbable sutures on
a long blunt needle. Take deep bites of splenic tissue on either side of the
tear, and tie the sutures snugly. Use omentum or Teflon buttresses to
prevent the stitches cutting through, together with a topical haemostatic
agent to control surface bleeding.
33.
MESH
• In openmethod in trauma, absorbable mesh is wrapped around
completely. It is partly haemostatic and creates tamponade also. Diff
erent methods are there to place the mesh as a wrap. Mesh may be
wrapped around completely and at the hilar level it is bunched loosely
using purse string suture.
• Another method, a large absorbable mesh is taken. At its centre, a
circular gap is made through which poles of the spleen are slid and mesh
is wrapped from hilum outwards; mesh margins are sutured on the
parietal surface of the spleen.
34.
PARTIAL SPLENECTOMY
• Forpartial splenectomy, fully mobilize the organ and carefully dissect in the
splenic hilum to identify and ligate the segmental arteries and veins. Incise
the capsule of the spleen at the line of ischaemia and use a finger-fracture
technique to resect the upper or lower pole. Secure haemostasis by means of
synthetic absorbable sutures or with argon coagulation. Preserve at least 30%
of the spleen volume to maintain adequate splenic function.
36.
POST OPERATIVE
• Checkthe haemoglobin, white cell and platelet counts postoperatively. Leucocytosis
and thrombocythaemia with peaks at 7–14 days.
• Persistent leucocytosis and pyrexia suggest the possibility of a subphrenic abscess.
• After an emergency splenectomy, vaccinate the patient one fully recovered
• Monitor the haemoglobin level
37.
COMPLICATION
• Intra operative- bleeding. Small splenic tears may be controlled with compression by
surrounding tissues and haemostatic diathermy or get control of the hilar vessels
• Postoperative haemorrhage is reported to occur in 2–5% of patients after splenectomy
bleeding. The usual sites are the hilar or short gastric vessels: require re laparotomy
• Thrombocytosis can occur following splenectomy, leading to deep venous thrombosis and
pulmonary emboli
• Respiratory complications such as pneumonia, atelectasis, and pleural effusion are by far
the most common morbidity following open splenectomy, occurring in 20–40% of patients
38.
• Injury toadjacent organs: the splenic flexure of the colon, the greater curvature of
the stomach and the tail of the pancreas are all susceptible to damage during
splenectomy. Undetected pancreatic injury may later present as pancreatic ascites, a
subphrenic collection or pancreatic fistula.
• Accessory spleens are noted in 15–30% of patients and account for late failure of
splenectomy in ITP.
39.
• Subphrenic collection:this may develop due to minor bleeding or serous
oozing from the raw area in the diaphragm and retroperitoneum. If this
happens, carefully monitor the platelet count and clotting parameters. A
CT (computed tomography) scan is often required to confirm the
diagnosis trauma.
• A subphrenic collection can usually be drained percutaneously with
antibiotic cover but may occasionally require a laparotomy.
• 4%
40.
OVERWHELMING POST-SPLENECTOMY INFECTION
(OPSI)
•As there is reduced IgM, tuftin, properdin and other antibodies, phagocytosis of
encapsulated bacteria is defective. So, the postsplenectomised patient is more prone
for Pneumococcal septicaemia (commonest), N. meningitides, H. infl uenzae and
Babesia microti infections
• Splenectomy there is a 1–2.5% risk of developing overwhelming septicaemia from
encapsulated bacteria, usually within 2 years of operation. The risk is higher in young
children (4–10%) and after splenectomy for haematological disease adults. The
mortality rate of post-splenectomy sepsis is higher in children (50%)
• Features—Prodromal phase—fever, chills, sore throat; hypotension, shock; DIC;
respiratory distress, coma, death
41.
PREVENTION
• Prompt medicalattention, particularly for respiratory illness. Patients should
be advised regarding immunization and foreign and to carry an information
card at all times.
• All patients should be advised to have yearly influenza immunization.
• Vaccination
#4 Up to 10% of splenectomies performed are secondary to iatrogenic injury.
#6 10 mm port is umbilical for camera; 5 mm left hand working port is between epigastrium and camera; 10 mm right hand working port is at left midclavicuar line, if endovascular stapler is being used this port should be 12 mm; 5 mm epigastric port for retraction of the stomach; left anterior axillary line 5 mm port when needed to retract spleen
#26 Consider injecting 1 ml of 1: 10 000 adrenaline (epinephrine) into the splenic artery immediately before ligating it. This can shrink the size of a massive spleen and facilitate the subsequent dissection. Post – like lap , ant as mentioned. Trauma – pack then resuscitate the start
#38 A colonic or stomach injury should be closed using interrupted seromuscular absorbable sutures. Injury to the tail of pancreas may require either primary repair or resection