Downloaded 201 times





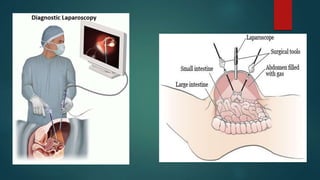







This document provides an overview of minimal access surgery (MAS). It defines MAS as applying modern technology to minimize surgical trauma without compromising exposure or safety. The history of MAS is traced from early laparoscopic procedures in the 1900s to developments like natural orifice transluminal endoscopic surgery (NOTES) and single incision laparoscopic surgery (SILS) more recently. The advantages of MAS include reduced pain, wounds, and recovery time compared to open surgery. Potential complications include injuries and those related to pneumoperitoneum such as arrhythmias. A variety of endoscopic, laparoscopic, and catheter-based minimal access procedures across several specialties are described in the document.



































































