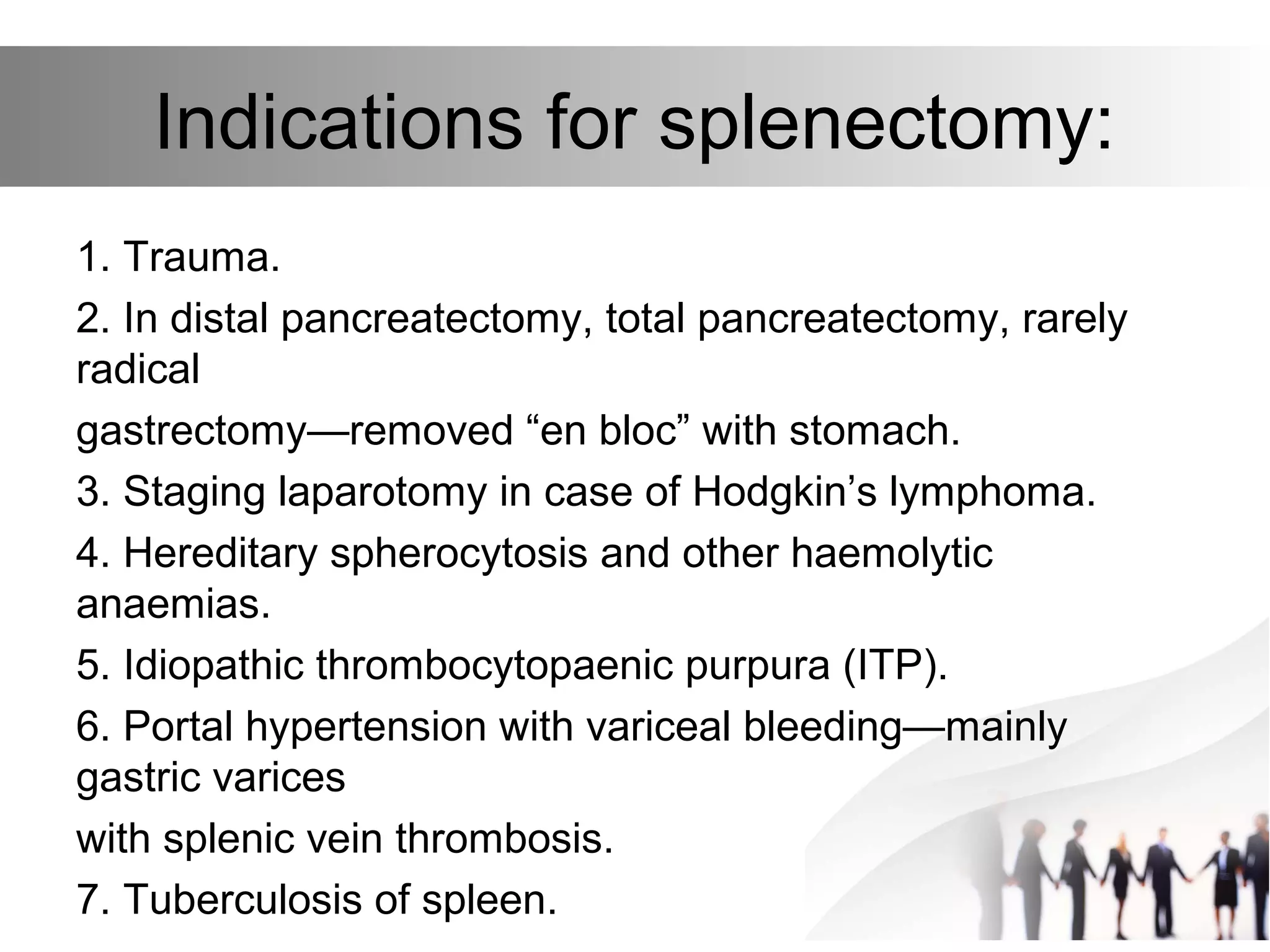
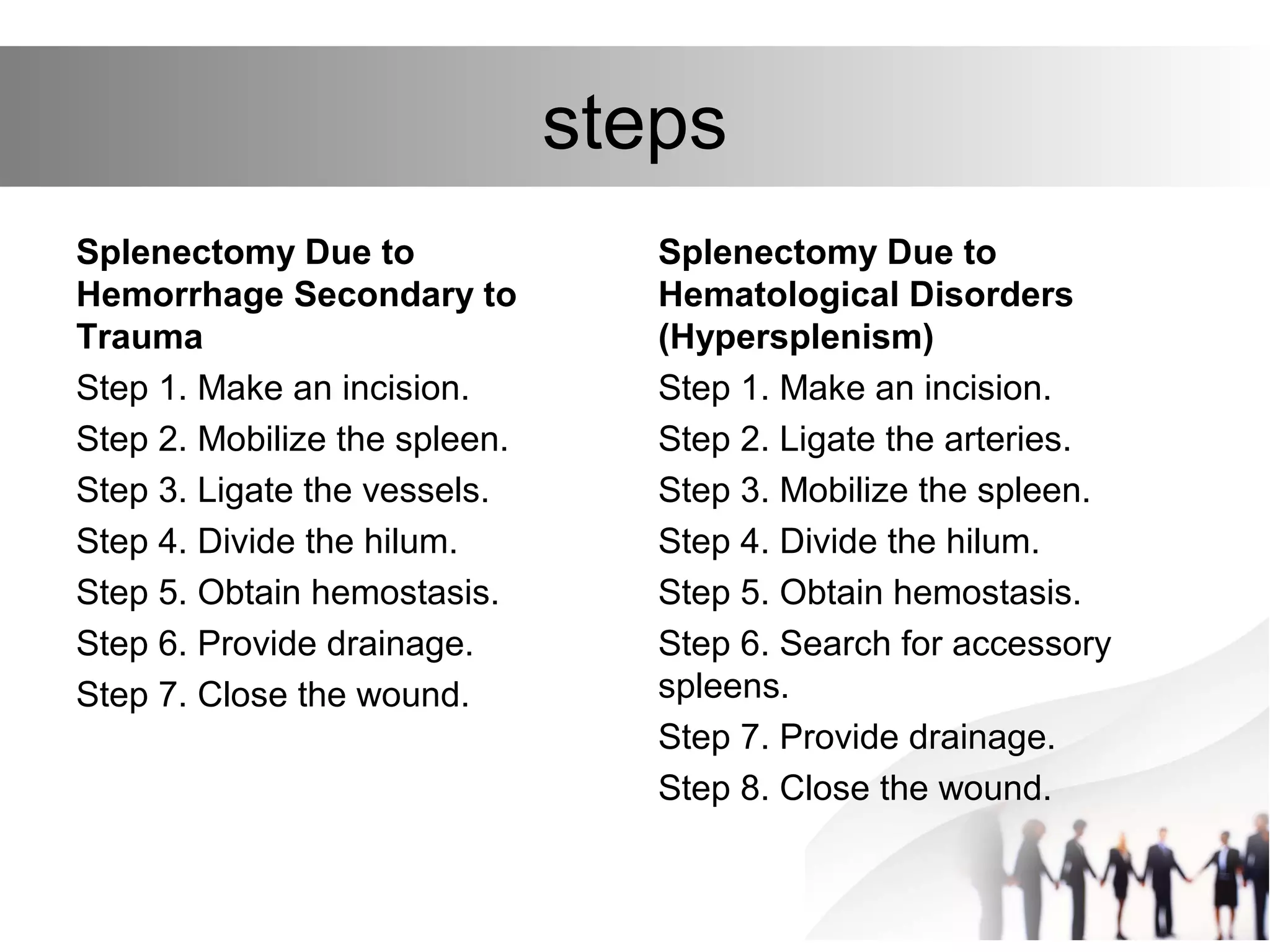
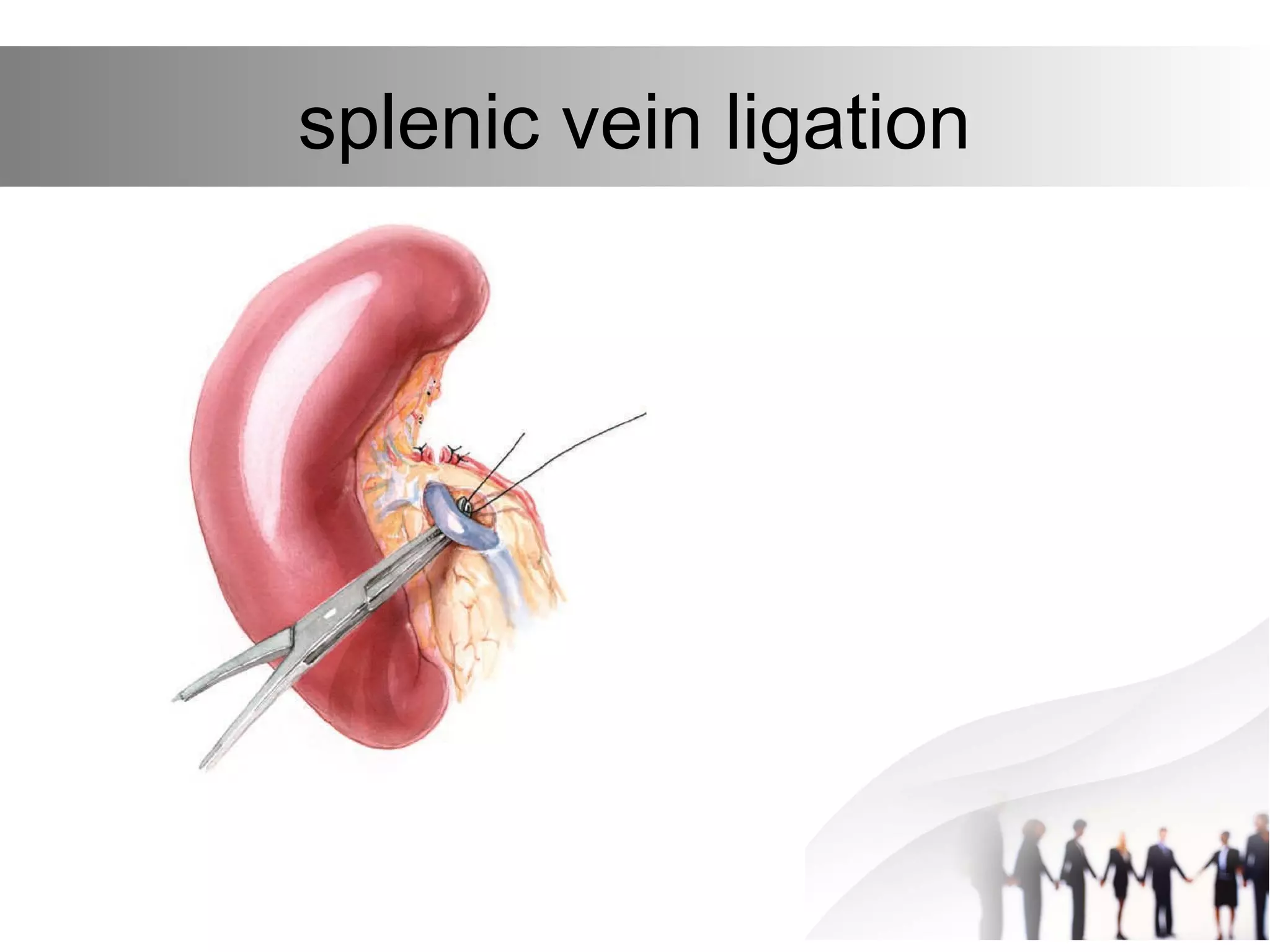
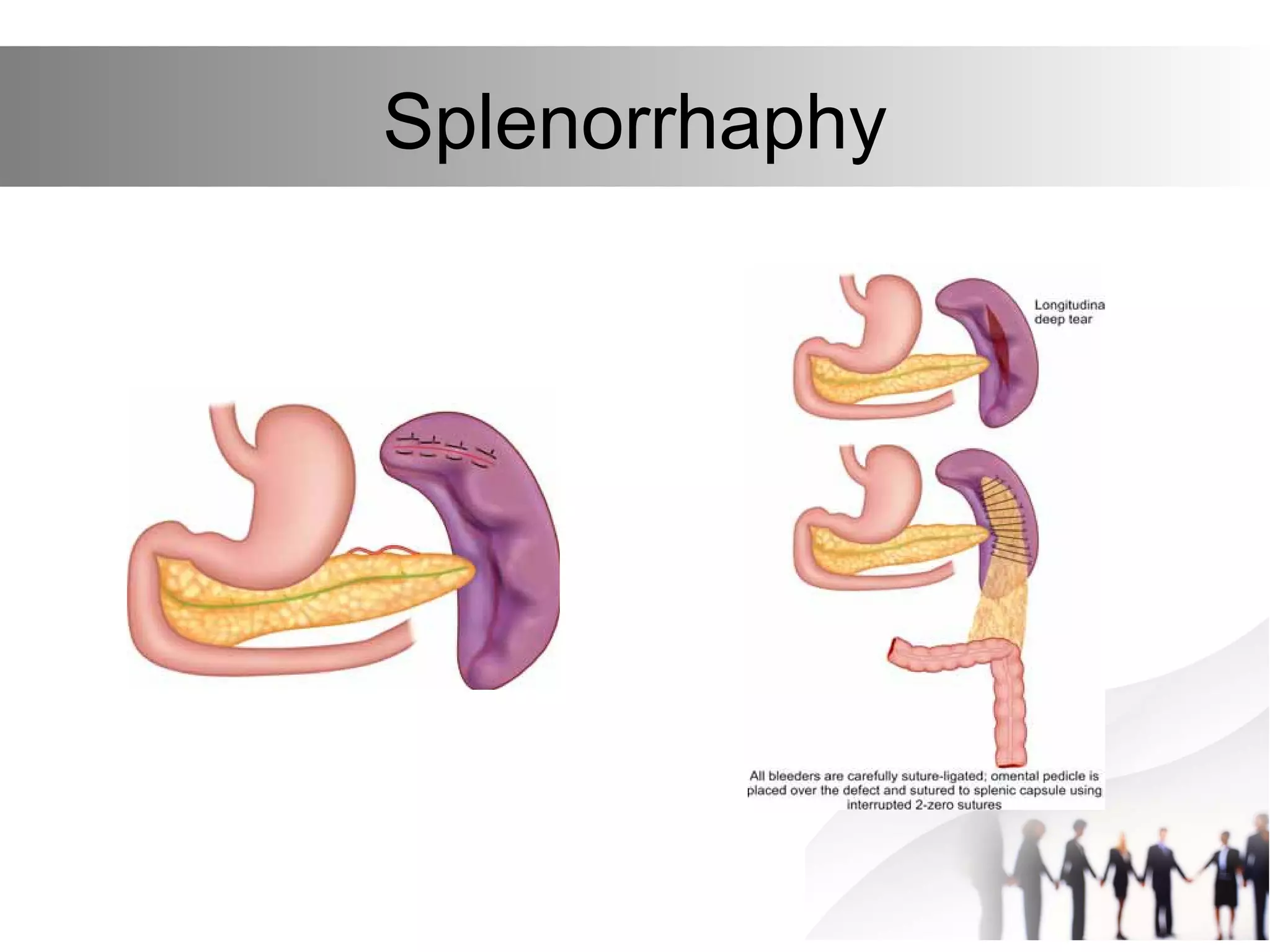
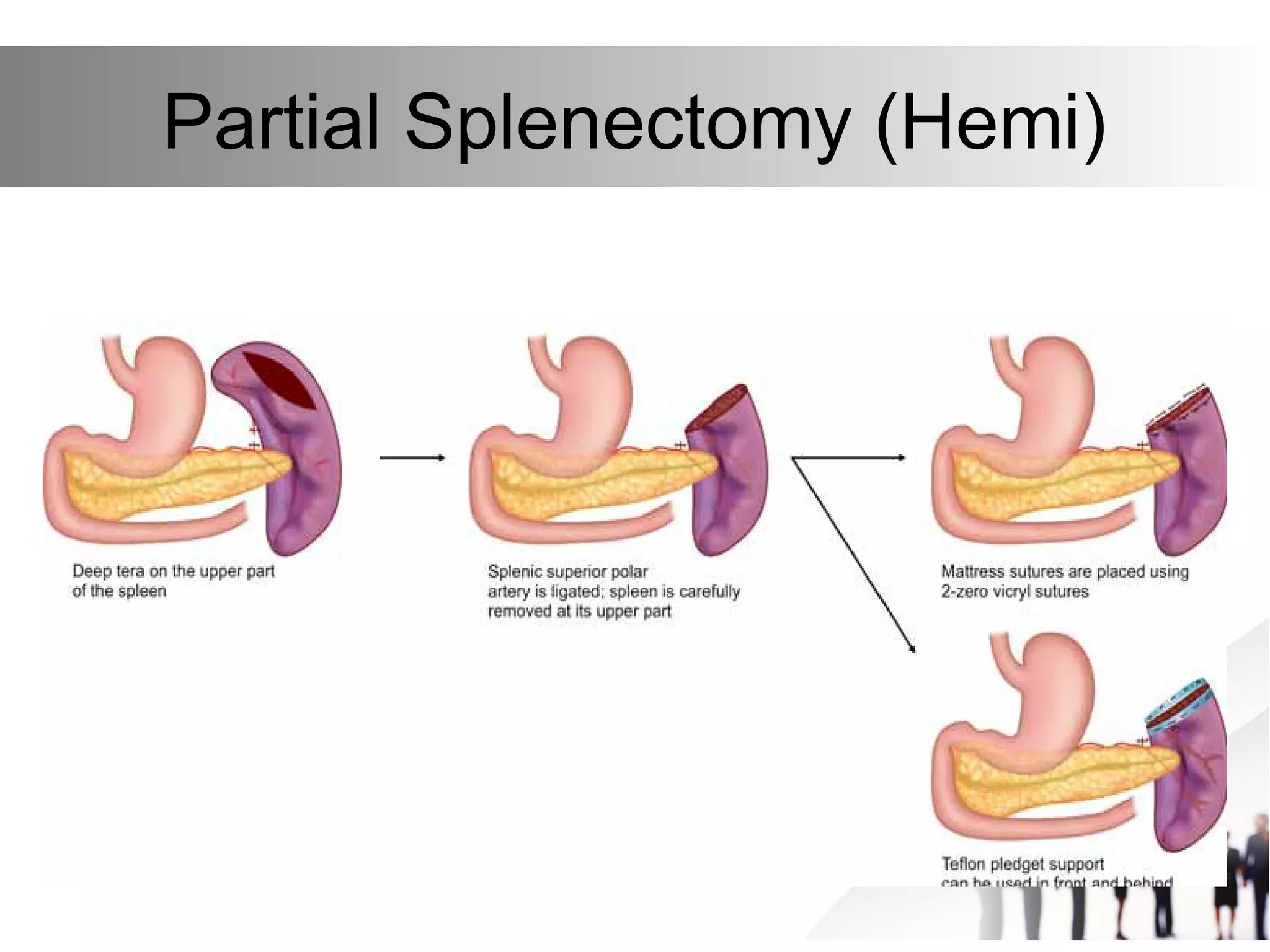
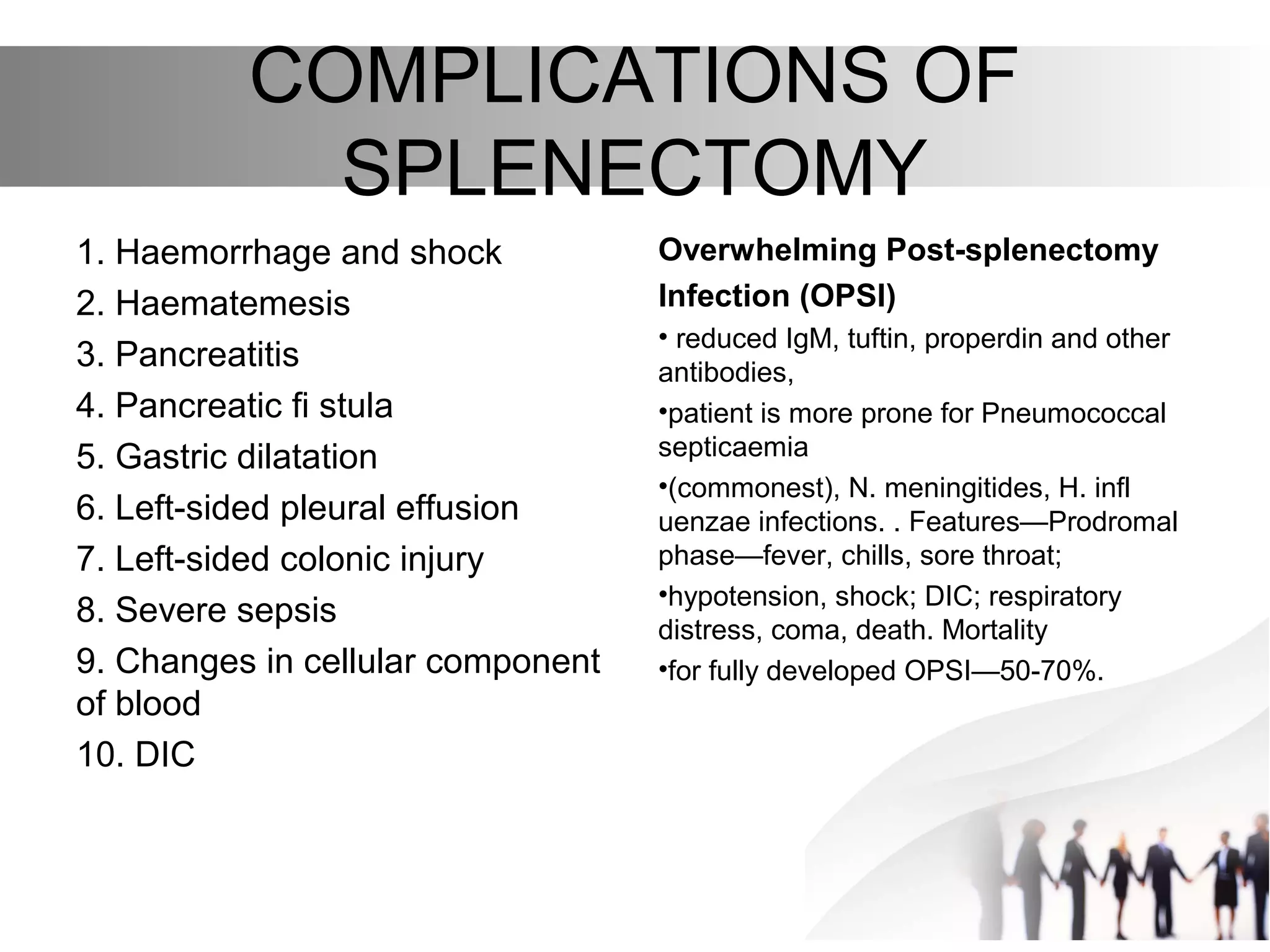
This document discusses splenectomy, including indications for the procedure, pre-operative preparation, surgical steps, incisions, mobilization techniques, vessel ligation, and postoperative care. It also covers splenic preservation surgeries such as partial splenectomy and laparoscopic splenectomy. Complications of splenectomy that are mentioned include hemorrhage, pancreatitis, infections like pneumococcal sepsis, and overwhelming post-splenectomy infection.